Clear Sky Science · en
Case-matched comparison of combined phacoemulsification with ab-interno trabeculectomy via Kahook dual blade and trabectome in a Caucasian population
Why this matters for everyday eye health
Glaucoma is a leading cause of irreversible blindness, and many people with this disease also develop cataracts as they age. Surgeons now have several ways to treat both problems in a single operation, but it is not always clear which option is best. This study asks a practical question that matters to patients, doctors, and health systems alike: when cataract surgery is combined with one of two modern glaucoma procedures, do the results really differ, or are the options essentially equivalent?
Two new tools for lowering eye pressure
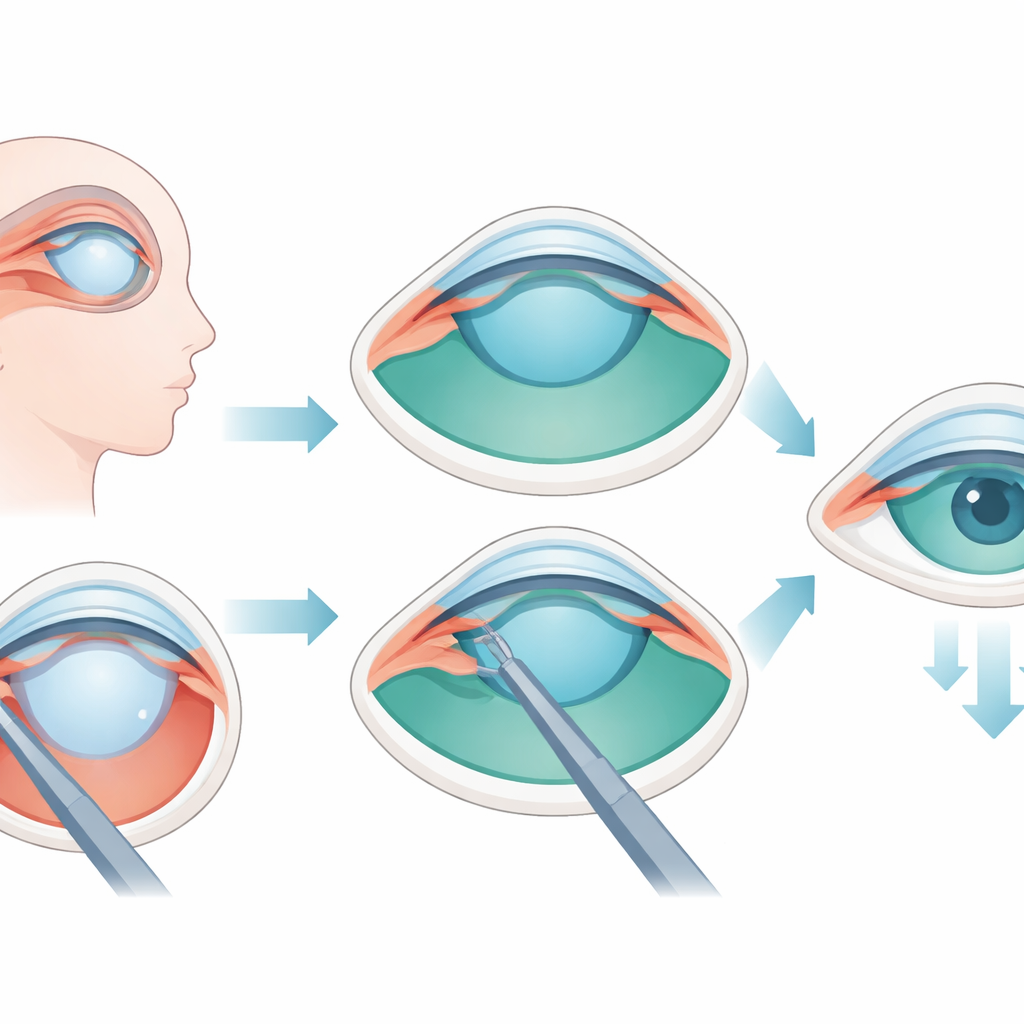
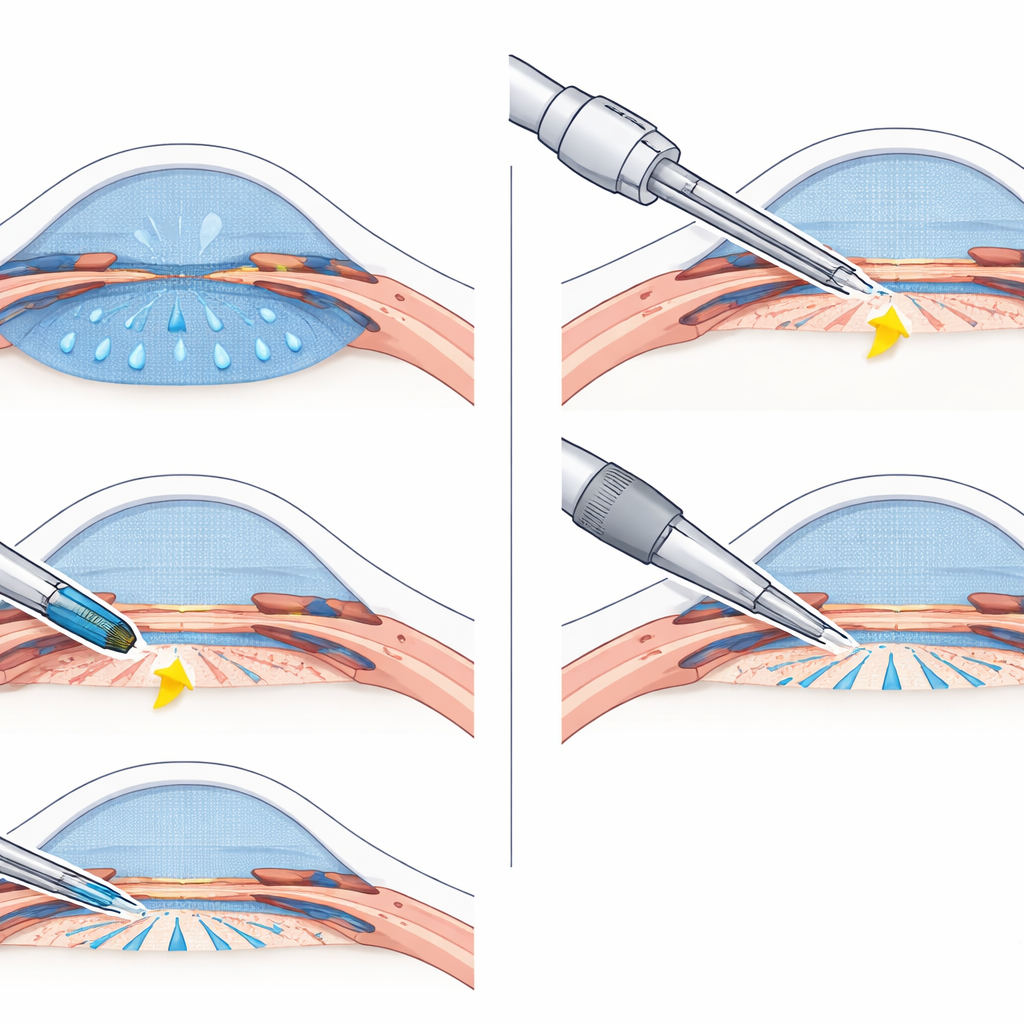
Glaucoma slowly damages the optic nerve, often because the clear fluid inside the eye cannot drain away easily, raising eye pressure and threatening sight. In recent years, so‑called microinvasive glaucoma surgery has offered gentler alternatives to older, more aggressive operations. Two common techniques, the Trabectome and the Kahook Dual Blade, work from inside the eye to remove a strip of the tissue that resists fluid outflow, opening a pathway into a circular drainage channel. Both can be performed through the same small cut used for cataract surgery, allowing surgeons to replace the cloudy lens while also reducing eye pressure.
Designing a fair head‑to‑head comparison
The researchers looked back at records from two German eye centers and identified people of Caucasian ethnicity who had cataract surgery combined with either the Trabectome or the Kahook Dual Blade. They focused on three common types of glaucoma and excluded other serious eye diseases that could cloud the results. To make the comparison fair, they matched 30 eyes in each group so that starting eye pressure, past highest pressure, use of pressure‑lowering drops, extent of optic nerve damage, vision, age, type of glaucoma, and length of follow‑up were all closely aligned. On average, patients were followed for about two years after surgery.
How success was measured
Because glaucoma care revolves around long‑term control of eye pressure, the team tracked pressure readings and medication use at the latest follow‑up visit. They used three increasingly strict definitions of success that reflected both how low the pressure fell and how much it dropped from the starting level, and they counted any need for further glaucoma surgery as a failure. They also recorded common side effects such as bleeding in the front of the eye, swelling at the back of the eye, and signs of inflammation, and they used standard statistical tests and survival curves to compare how often each procedure met the chosen targets over time.
What the study found in real patients
Both surgical combinations performed remarkably alike. Average eye pressure fell by about 29 percent in each group, from roughly 20 millimeters of mercury before surgery to about 14 afterward, and these gains were maintained over nearly two years. Patients in both groups needed slightly fewer glaucoma drops after surgery, and the chances of meeting each of the three success definitions were similar. Serious complications such as severe infection or retinal detachment did not occur in either group. The main difference was that mild bleeding in the front of the eye was more common after the Kahook Dual Blade, although this did not translate into long‑term harm.
What this means for people facing surgery
For patients of Caucasian background undergoing cataract surgery with coexisting glaucoma, this study suggests that adding either the Trabectome or the Kahook Dual Blade offers comparable pressure‑lowering benefit and safety. In other words, from the standpoint of preserving vision and reducing the burden of eye drops, the two options appear equally reasonable in this setting. That leaves room for practical considerations—such as surgeon experience, equipment costs, and local availability—to guide the final choice. As larger, long‑term trials emerge, they may refine these conclusions, but for now patients can be reassured that both approaches are solid, evidence‑based ways to protect their sight.
Citation: Kiessling, D., Bleiel, H., Roessler, G.F. et al. Case-matched comparison of combined phacoemulsification with ab-interno trabeculectomy via Kahook dual blade and trabectome in a Caucasian population. Sci Rep 16, 8944 (2026). https://doi.org/10.1038/s41598-026-39331-8
Keywords: glaucoma surgery, cataract and glaucoma, microinvasive glaucoma, eye pressure control, Kahook versus Trabectome