Clear Sky Science · en
A 15-year registry based follow up study of site specific cancer mortality among immigrants with type 2 diabetes in Sweden
Why this matters for people with diabetes
As type 2 diabetes becomes more common worldwide, cancer is emerging as one of the leading causes of death for people living with the disease. At the same time, many European countries, including Sweden, have large and growing immigrant populations who often face extra hurdles in healthcare. This study asks a simple but important question: among people with type 2 diabetes in Sweden, do immigrants die from cancer at different rates than people born to Swedish parents—and does this change depending on where they come from and how long they have lived in Sweden?
Looking at hundreds of thousands of patients
The researchers used Sweden’s detailed national health and population registers to follow 478,607 adults who were diagnosed with type 2 diabetes between 2006 and 2021. They tracked deaths from all cancers combined and from eight specific cancers that are often linked to diabetes, including cancers of the liver, pancreas, bowel, kidney, bladder, breast, and the lining of the womb (endometrium). People were grouped as native Swedes, first-generation immigrants (born abroad) and second-generation immigrants (born in Sweden with at least one foreign-born parent). For first-generation immigrants, the team also considered age at arrival in Sweden and how many years they had lived in the country when their diabetes was diagnosed.
A surprising advantage for many first-generation immigrants
Despite often having lower incomes and more barriers to care, first-generation immigrants with diabetes generally had the same or lower cancer death rates as native Swedes. This was especially true for immigrants from non-Western regions such as Asia, Africa, the Middle East and Latin America, who showed notably lower mortality for several cancers including pancreas and bowel. One possible explanation is the so-called “healthy migrant effect,” where people who move country are, on average, healthier than those who stay behind. Differences in lifestyle before migration and patterns of diabetes treatment, such as higher use of the drug metformin, may also play a role. However, the study could not directly test these explanations because it lacked detailed data on smoking, diet and specific medications.
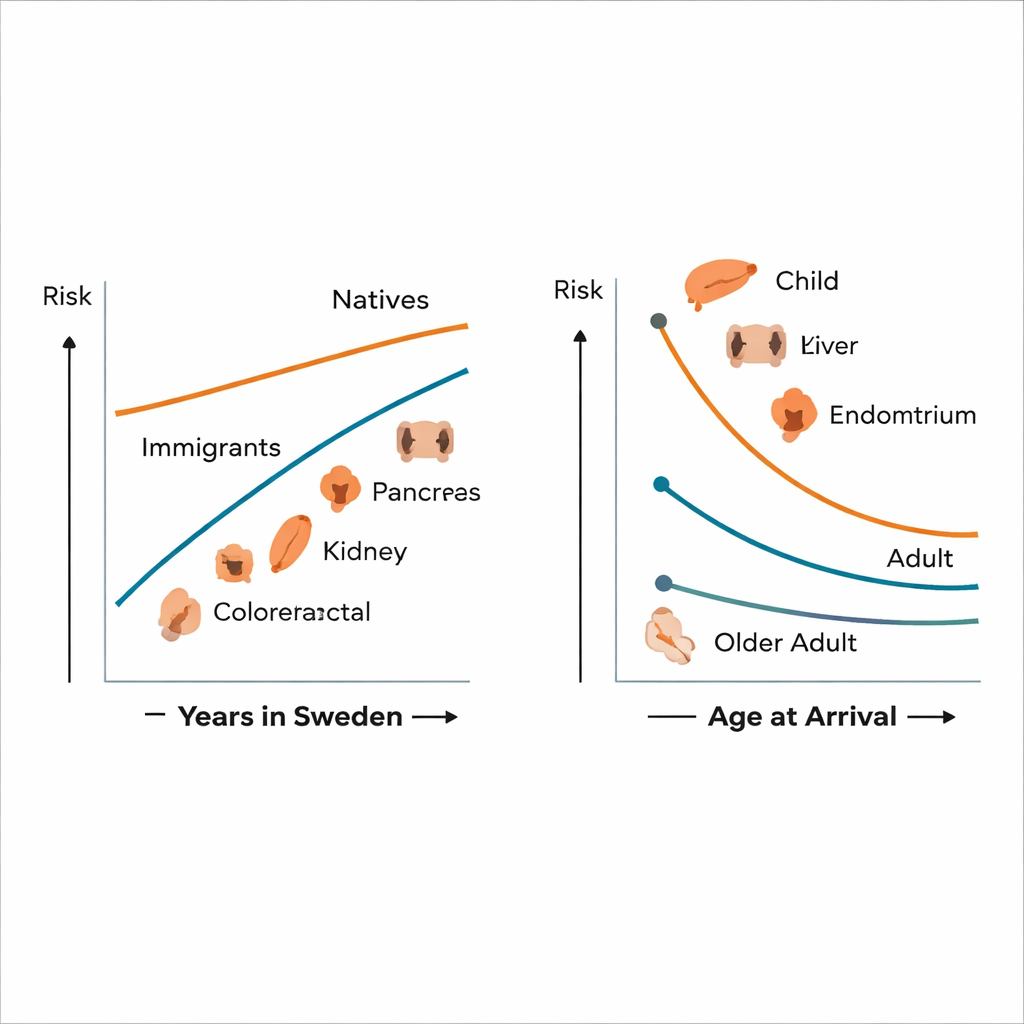
When and how people migrate makes a difference
The study found that not all immigrant groups shared this advantage. Among first-generation immigrants who arrived in Sweden before age 18, cancer death risks for several sites—including bowel, liver, pancreas, kidney and bladder—tended to be higher and closer to, or even above, those of native Swedes, although many differences were not statistically certain. For those who arrived as adults, cancer mortality was more often lower. Over time, as immigrants lived longer in Sweden, their overall cancer death rates gradually moved toward the levels seen in natives. For bowel and pancreatic cancer in particular, immigrants who had lived in Sweden for 15 years or more at the time of diabetes diagnosis had about 35–40% higher mortality than those with shorter stays. This pattern suggests that adopting aspects of Western lifestyle and environment, along with changing access to screening and care, may erode any early health advantage.
Second-generation immigrants lose some protection
For people born in Sweden to immigrant parents, cancer mortality patterns looked more similar to those of native Swedes. Overall death rates from cancer were not markedly different, but there were important exceptions. Second-generation individuals with Western parental origins had higher death rates from kidney cancer, and those with Nordic parental origins had higher mortality from endometrial cancer, compared with natives. Since these groups grew up entirely in Sweden, their risks may reflect a mix of inherited vulnerability, early-life conditions such as low birth weight, and social and economic disadvantages, along with the added impact of diabetes-related kidney damage and hormonal changes.
What this means for care and prevention
For the average reader, the main takeaway is that cancer risk among people with type 2 diabetes is not the same for everyone, and it can change across generations of immigrants. Many first-generation immigrants currently show lower cancer death rates, but this advantage appears to fade the longer they live in Sweden and across their children’s generation, with some cancers even becoming more deadly. The authors conclude that health systems should not treat diabetes and cancer in isolation. Instead, they call for better-integrated care that routinely considers cancer prevention and early detection in diabetes clinics, together with culturally tailored support for immigrant patients. Such efforts—especially targeted toward high-risk groups like early-arriving migrants and second-generation individuals with Western or Nordic roots—could help reduce avoidable deaths and make the promise of universal healthcare more of a reality.
Citation: Tollosa, D.N., Juarez, S.P., Grotta, A. et al. A 15-year registry based follow up study of site specific cancer mortality among immigrants with type 2 diabetes in Sweden. Sci Rep 16, 6493 (2026). https://doi.org/10.1038/s41598-026-39293-x
Keywords: type 2 diabetes, cancer mortality, immigrants, Sweden, health disparities