Clear Sky Science · en
Preheating colistimethate sodium enhances its efficacy against multi/extensively drug-resistant Gram-negative bacilli in preservation fluid
Why this matters for transplant patients
When someone receives a lifesaving organ transplant, the donated organ spends hours in a chilled preservation liquid before surgery. That liquid can sometimes carry dangerous, highly drug-resistant bacteria, which may cause severe infections in already fragile patients. This study explores a surprisingly simple idea: slightly "cooking" a common last‑resort antibiotic before adding it to the preservation fluid, to see if this makes it much better at killing those hard‑to‑treat germs without harming the organ.
Hidden germs in the cold storage bath
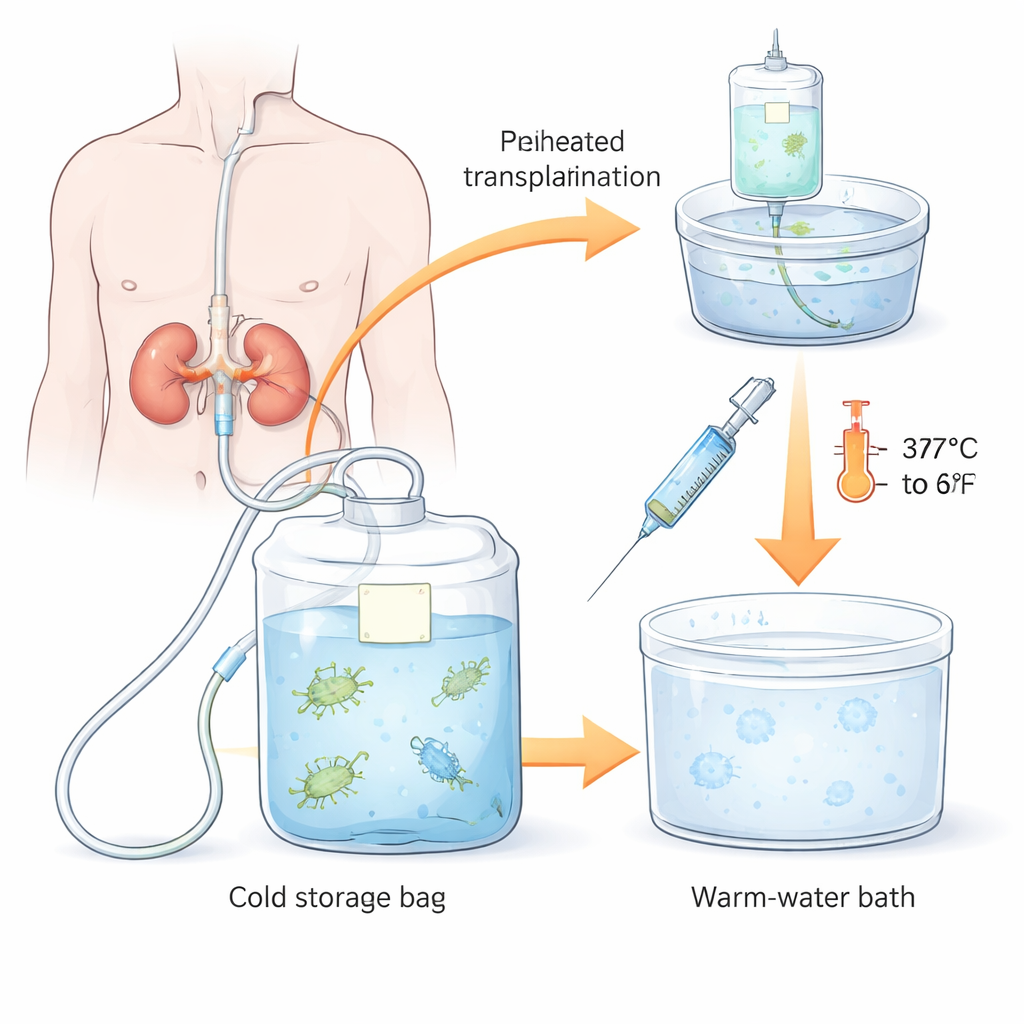
Transplanted organs, such as kidneys, are flushed and stored in a special preservation fluid while being transported from donor to recipient. Studies show that this fluid is often contaminated with microbes, especially a group called Gram‑negative bacteria, which includes notorious hospital bugs like Pseudomonas, Klebsiella, Escherichia coli and Acinetobacter. Many of these strains are now multidrug‑resistant or extensively drug‑resistant, meaning they shrug off most of our standard antibiotics. Although not every contaminated fluid causes infection, when these resistant germs are transmitted to a transplant recipient, the consequences can include longer intensive care stays, kidney damage, graft loss, and even death.
A last‑resort drug with a temperature twist
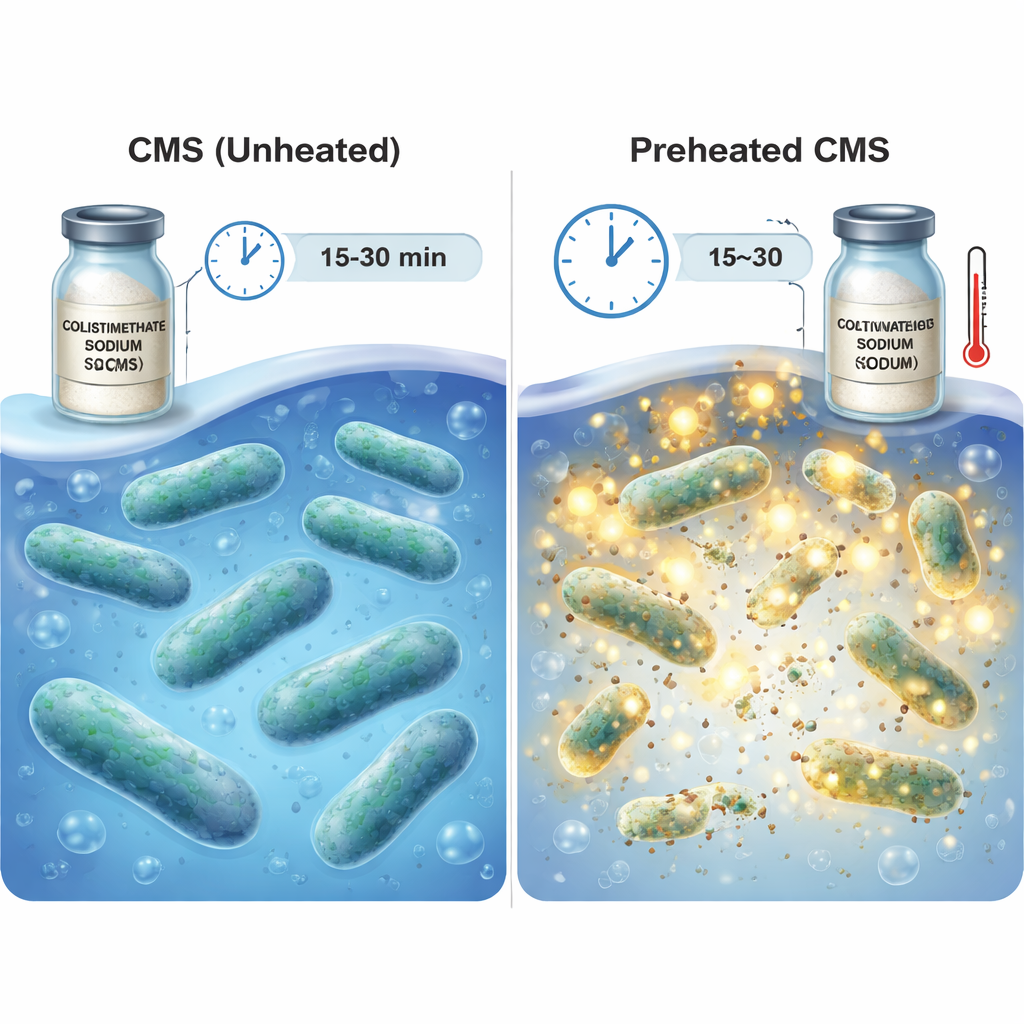
The researchers focused on colistimethate sodium (CMS), a widely available hospital drug used as a last‑line treatment against multidrug‑resistant Gram‑negative bacteria. CMS itself is a "pro‑drug"—it must slowly break down into colistin, the truly active substance that attacks bacterial outer membranes. This conversion normally happens over many hours at body temperature. The team wondered if they could speed up that activation step by gently heating CMS in solution before cooling it again and adding it to the organ preservation fluid. They tested various combinations of temperature (37 °C versus 60 °C) and heating times (5 to 30 minutes) under conditions that mimic static cold storage of organs at near‑freezing temperatures.
Preheating sharply boosts bacterial kill
In laboratory experiments, the team challenged preheated CMS with five real‑world hospital strains: four Gram‑negative, drug‑resistant strains—carbapenem‑resistant Pseudomonas aeruginosa, Klebsiella pneumoniae, E. coli and Acinetobacter baumannii—and one Gram‑positive strain, methicillin‑resistant Staphylococcus aureus (MRSA). After three hours in cold conditions resembling organ storage, they counted surviving bacteria. Heating CMS at 60 °C for 15–30 minutes led to dramatic reductions in all four Gram‑negative strains: some were almost completely wiped out, with average inhibition rates approaching or reaching 100%. Lower‑temperature heating at 37 °C helped only modestly and only after longer times, and it was far less reliable. MRSA, which has a different cell wall structure, remained unaffected, matching what is known about colistin’s limited activity against Gram‑positive bacteria.
Checking safety for the kidney
Because polymyxin‑type drugs like colistin can damage kidneys when given to patients for days, the scientists also asked whether their preheated CMS mixture would harm kidney cells over the shorter window that donor organs are stored on ice. They exposed human kidney tubule cells to preheated CMS at cold temperatures for 3, 6, or 18 hours. For up to 6 hours—the time frame most relevant to organ transport—the cells looked normal under the microscope and showed no meaningful drop in viability compared to untreated cells. Only after 18 hours of continuous exposure did clear signs of cell injury appear, suggesting that brief, single‑dose use in preservation fluid may be much safer than prolonged treatment in living patients.
Where this could lead for transplants
To a layperson, the key message is that a simple heat‑and‑cool step applied to an existing antibiotic can greatly improve its ability to clean up the liquid that surrounds a donor organ during transport. Preheating CMS at 60 °C for 15–30 minutes, then adding it to the preservation fluid, rapidly kills many of the most feared drug‑resistant Gram‑negative bacteria in the lab, without obvious short‑term harm to kidney cells under cold‑storage conditions. If future studies confirm these findings in actual transplant settings and refine the best temperature‑time recipe, this low‑tech adjustment could reduce early post‑transplant infections and help make scarce donor organs safer and more usable.
Citation: Tang, D., Zhang, L., Duan, Y. et al. Preheating colistimethate sodium enhances its efficacy against multi/extensively drug-resistant Gram-negative bacilli in preservation fluid. Sci Rep 16, 7523 (2026). https://doi.org/10.1038/s41598-026-38748-5
Keywords: organ transplantation, drug-resistant bacteria, preservation fluid, colistin, antibiotic preheating