Clear Sky Science · en
Correlation analysis of chest HRCT quantitative parameters, exhaled nitric oxide, and pulmonary function in patients with chronic obstructive pulmonary disease
Why this lung study matters
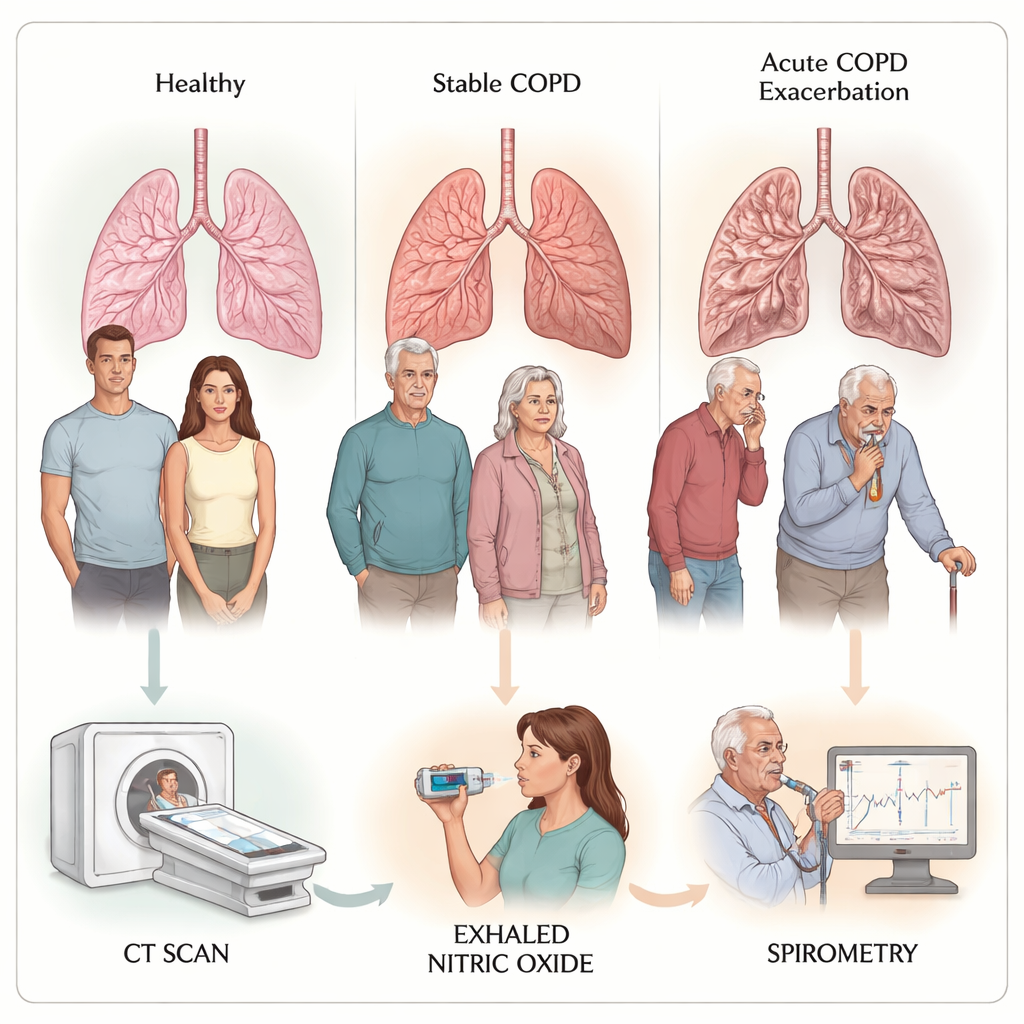
Chronic obstructive pulmonary disease (COPD) is a leading cause of illness and death worldwide, often linked to long-term smoking or air pollution. People living with COPD frequently wonder why their breathing suddenly worsens during flare-ups, and doctors are searching for better ways to spot early damage and track the disease without relying only on exhausting breathing tests. This study looks at three different windows into the lungs—detailed CT scans, a simple breath test for nitric oxide, and standard lung function tests—to see how they fit together and what they reveal about hidden damage in the smallest airways.
Peeking inside the lungs in three ways
The researchers followed 115 people hospitalized for sudden COPD flare-ups, 89 people with stable COPD seen in clinic, and 70 healthy volunteers. All participants had a high-resolution CT scan of the chest, which can measure how thick the airway walls are and how much of the lung looks like emphysema (over-inflated, fragile air sacs). They also performed standard breathing tests that measure how much air a person can forcefully blow out, and they used a handheld device to measure nitric oxide in exhaled breath. Nitric oxide is a gas naturally produced in the airways and can serve as a sign of inflammation.
Small tubes, big changes
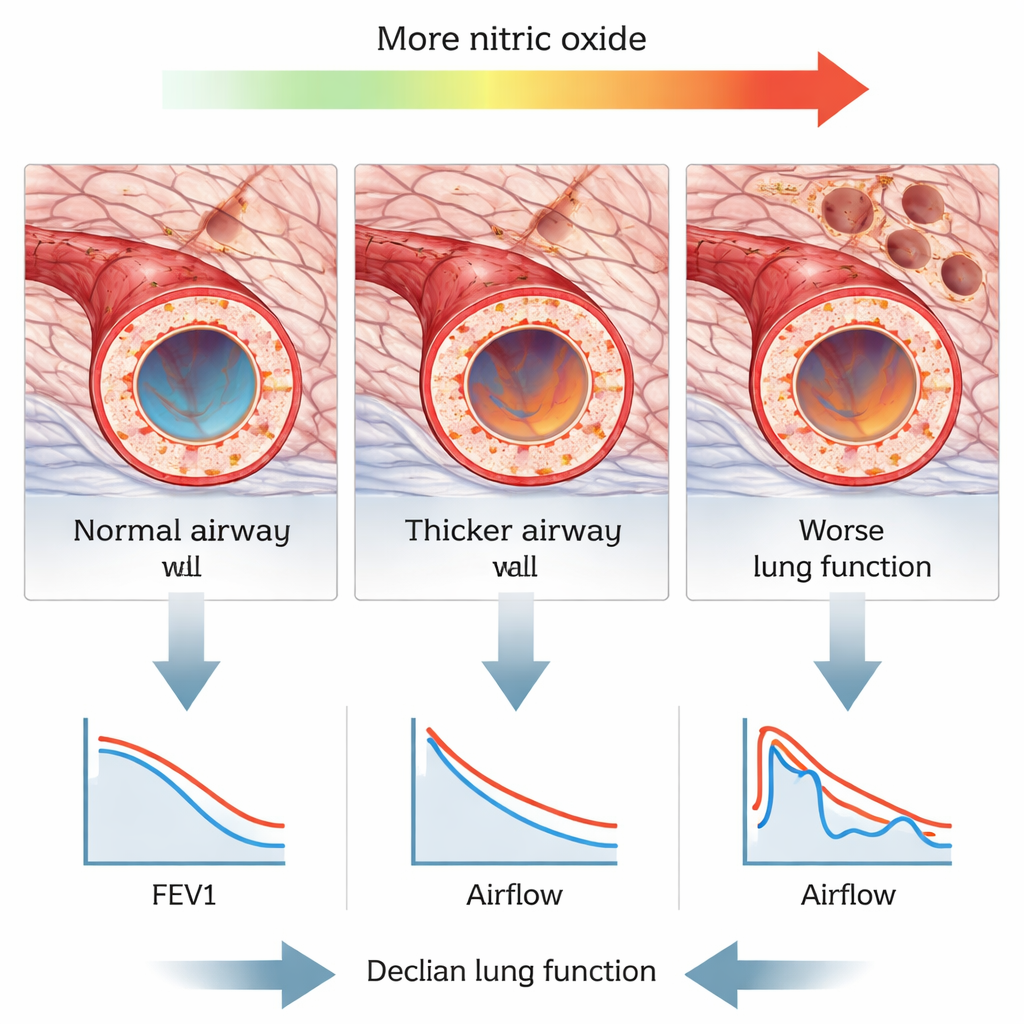
The team focused on very small breathing tubes in the right upper lung, where measurements are technically easier and more reliable. Compared with people whose COPD was stable, patients having an acute flare showed thicker airway walls when corrected for body size and a larger ratio of wall thickness to the nearby lung artery. When the COPD groups were compared to healthy volunteers, both stable and flare-up patients had thicker walls and higher ratios of wall thickness to airway width, clear signs of “remodeling” in the tiny airways. These changes were present even when CT measures of emphysema (the proportion of very low-density lung, called LAA−950%) were similar between stable and flare-up groups, suggesting that small airway damage can worsen without a major jump in visible emphysema.
Inflammation signal in a breath
Not all nitric oxide measurements told the same story. The common test at a gentle flow (FeNO50), which mainly reflects larger airways, did not consistently track with CT changes or lung function. But when people exhaled faster (FeNO200), and especially when the researchers estimated nitric oxide coming from the air sacs themselves (a value called CaNO), the results lined up strongly with structural damage. Higher FeNO200 and CaNO were linked to thicker airway walls and a higher wall-to-artery ratio—markers of remodeling in the small airways. CaNO also rose as the CT emphysema score increased. At the same time, higher FeNO200 and CaNO were tied to worse scores on breathing tests, including how much air could be blown out in one second and how well small airways stayed open during exhalation.
Connecting structure, inflammation, and breath tests
CT measurements of airway wall thickness and certain size ratios were clearly related to how badly lung function had declined. Thicker walls and higher wall-to-diameter or wall-to-artery ratios went hand in hand with lower values on standard tests of airflow, especially those that highlight the performance of the smallest airways. The CT emphysema score also correlated with poorer lung function and tended to increase as patients moved from milder to more severe COPD stages. Together, these patterns paint a picture in which ongoing inflammation in the peripheral airways and air sacs thickens airway walls, narrows the breathing tubes, and gradually destroys lung tissue—changes that are picked up as higher exhaled nitric oxide, worse CT scores, and reduced airflow.
What it means for patients and care
For people living with COPD, this research suggests that a simple breath test, combined with detailed CT scanning, can provide a richer picture of lung health than breathing tests alone. In particular, nitric oxide measured at higher exhalation speeds and estimates from the lung’s air sacs may serve as convenient markers of hidden small-airway damage and emphysema. Doctors might one day use these markers to detect early disease, monitor flare-ups, and tailor anti-inflammatory treatment before permanent damage accumulates. In plain terms, the study shows that what you see on a scan, what you breathe out, and how well you blow into a tube are tightly linked views of the same underlying problem: inflamed, thickened, and fragile small airways that make every breath harder.
Citation: Shen, Y., Gu, JF., Shi, JF. et al. Correlation analysis of chest HRCT quantitative parameters, exhaled nitric oxide, and pulmonary function in patients with chronic obstructive pulmonary disease. Sci Rep 16, 7111 (2026). https://doi.org/10.1038/s41598-026-38579-4
Keywords: COPD, small airway remodeling, exhaled nitric oxide, chest CT, pulmonary function