Clear Sky Science · en
Comparing and combining xevinapant with ATR and PARP inhibition for the radiosensitization of HPV-negative HNSCC cells
Why boosting radiation matters
Radiation therapy is a mainstay treatment for cancers of the mouth and throat, but many tumors resist it, forcing doctors to use high doses that can damage normal tissues. This study asks a practical question with big implications for patients: among several modern cancer drugs designed to make tumor cells more vulnerable, which ones actually work best with radiation against tough, HPV‑negative head and neck cancers grown in the lab?
Current treatment and its limits
People with locally advanced head and neck squamous cell carcinoma are often treated with a combination of radiation and the chemotherapy drug cisplatin, or with surgery followed by radiation. While this approach can control cancer, it frequently leaves patients with serious long‑term side effects such as difficulty swallowing, dry mouth, hearing problems, and kidney damage. Many older or medically fragile patients cannot tolerate cisplatin at all. That has fueled intense interest in “radiosensitizers” – drugs that make tumor cells easier to kill with radiation so that treatment can be more effective or, potentially, gentler.
A promising drug that stumbled
One such drug, xevinapant, was initially hailed as a breakthrough. It mimics a natural protein called SMAC and blocks molecules that help cancer cells avoid programmed cell death. In earlier work, adding xevinapant to standard chemoradiation improved outcomes in a phase 2 clinical trial for head and neck cancer, raising hopes that it could become a new standard of care. But a much larger phase 3 trial, called TrilynX, was stopped early when interim data showed not only a lack of benefit but even worse survival and more side effects in the xevinapant group. That unexpected failure created an urgent need to reassess how well xevinapant truly helps radiation, and to compare it with other, newer strategies.
Putting three strategies head‑to‑head
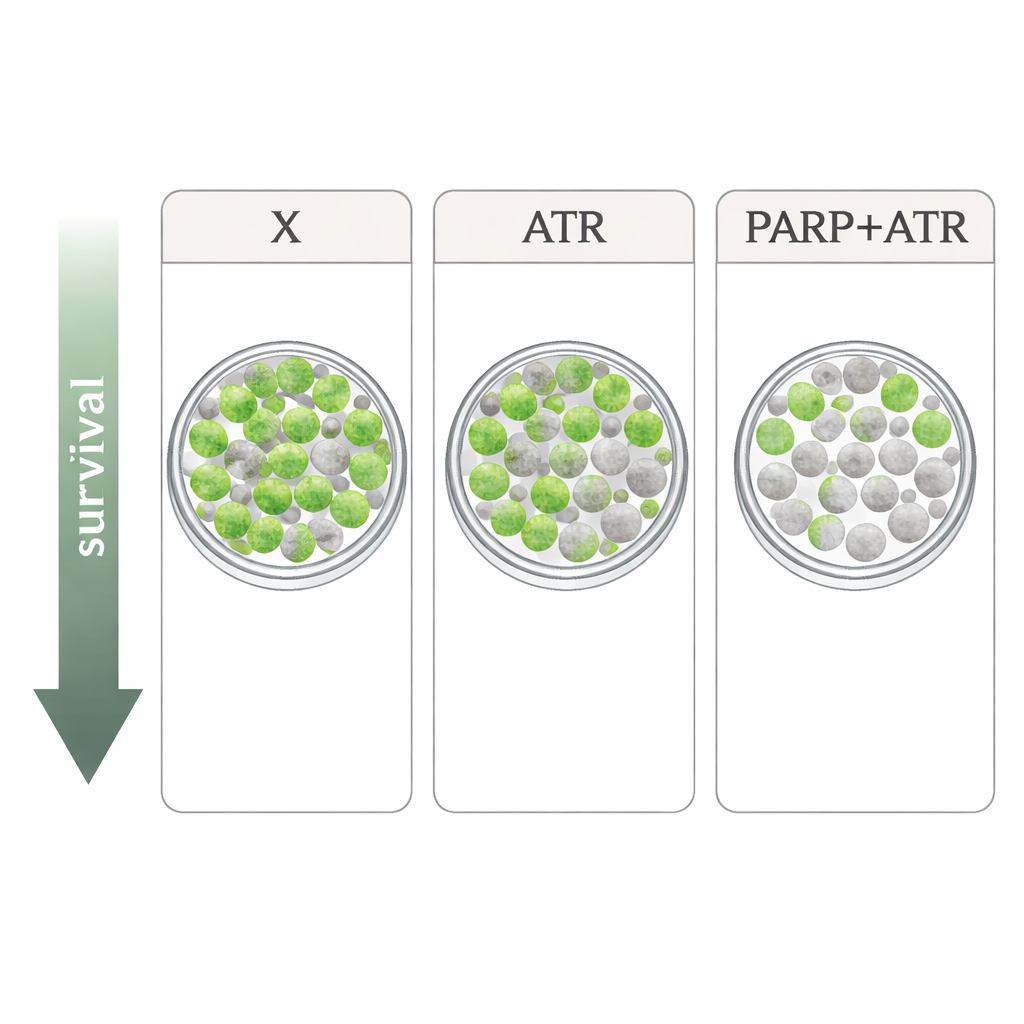
The researchers studied four radiation‑resistant HPV‑negative head and neck cancer cell lines. They compared xevinapant with two drugs that target the cell’s DNA damage response: the ATR inhibitor tuvusertib and the PARP inhibitor olaparib, both used at doses similar to those achievable in patients. ATR and PARP are key players that help cells pause the cell cycle and repair DNA after damage such as that caused by X‑rays. In simple growth tests, each drug alone slowed cell proliferation only modestly, and the patterns differed among cell lines. When combined with radiation in the most stringent assay—counting how many single cells can still grow into colonies—the picture sharpened: xevinapant gave only mild or no extra radiation effect in several lines, whereas both tuvusertib and olaparib consistently made radiation more lethal. The strongest impact came from combining ATR and PARP inhibition, which produced especially deep drops in colony survival in three of the four cell lines.
Cell death signals are not the whole story
Because xevinapant is designed to trigger cell death, the team also measured how many cells became apoptotic or lysed after treatment, with and without radiation. These death markers increased noticeably in some settings—particularly in one cell line called HSC4 and when drugs were combined—but did not reliably track with how well radiation actually suppressed long‑term survival. In other words, the short‑term death readouts were poor predictors of true radiosensitization. This mismatch underscores a key lesson for drug development: only assays that follow cells long enough to see whether they can regrow—such as colony formation tests—can properly judge whether a radiosensitizer is effective.
What this means for future treatments
From these lab experiments, xevinapant does have some ability to boost radiation in HPV‑negative head and neck cancer cells, but its impact was weaker and less consistent than approaches that directly interfere with DNA damage handling through ATR and PARP. Pairing ATR and PARP inhibitors together gave the most powerful effect, suggesting that carefully dosed combinations of these drugs with radiotherapy may offer a more promising path than further pursuing xevinapant, at least for this cancer type. Translating these findings to the clinic will not be straightforward, since such drugs can also stress normal, fast‑dividing tissues and have already required dose reductions in early trials. Still, the work points clinicians and researchers toward DNA repair–targeting strategies as more compelling candidates to make radiation therapy both more effective and, potentially, safer for patients who cannot receive standard chemotherapy.
Citation: Roehrle, J., Perugachi-Heinsohn, A., Gatzemeier, F. et al. Comparing and combining xevinapant with ATR and PARP inhibition for the radiosensitization of HPV-negative HNSCC cells. Sci Rep 16, 5882 (2026). https://doi.org/10.1038/s41598-026-38550-3
Keywords: head and neck cancer, radiation therapy, DNA repair inhibitors, xevinapant, radiosensitization