Clear Sky Science · en
Ketoacidosis at childhood type 1 diabetes onset negatively affects residual beta-cell functions during the first year after diagnosis
Why this matters for families
For many families, a child’s diagnosis of type 1 diabetes feels sudden and overwhelming. Some children arrive at the hospital already dangerously ill with a complication called diabetic ketoacidosis, or DKA. This study asks a simple but crucial question: does being that sick at diagnosis cause more lasting damage to the insulin-producing cells in the pancreas during the first year after diagnosis? The answer helps parents, doctors, and health systems understand why catching diabetes earlier can change a child’s long‑term health.
Two ways children first show up
Researchers in Poland followed 101 children aged 7 to 18 who were newly diagnosed with type 1 diabetes. About half of them arrived with DKA, meaning their bodies had run out of insulin so severely that acids built up in the blood. The other half had high blood sugar but did not have this dangerous complication. The team compared these two groups over the first year after diagnosis, looking at how much insulin the children needed each day, how well their blood sugar was controlled, and how much of their own natural insulin they were still making. 
Tracking the body’s own insulin
Instead of measuring insulin directly, the scientists focused on a partner molecule called C‑peptide, which is released whenever the body makes insulin. Higher C‑peptide levels mean the pancreas is still doing some of the work. The children drank a standardized nutrition shake at three time points—within two weeks of diagnosis, then at six and twelve months—while blood samples were taken to see how much C‑peptide their bodies produced in response. This test, called a mixed‑meal tolerance test, is considered a gold‑standard way to gauge how much life is left in the insulin‑producing cells.
What happened over the first year
At the start, children who arrived with DKA already had lower insulin and C‑peptide levels than those without DKA, even though their long‑term blood sugar marker (HbA1c) was similar. All children improved in blood sugar control after starting treatment, but important differences remained. Those who had DKA needed more injected insulin at almost every visit to reach similar HbA1c levels, suggesting their pancreas was contributing less. By six months, the gap in C‑peptide became clear: children with DKA had substantially lower C‑peptide responses than those without, and this disadvantage persisted at twelve months. In other words, the insulin‑making cells in the DKA group appeared more damaged and continued to decline faster. 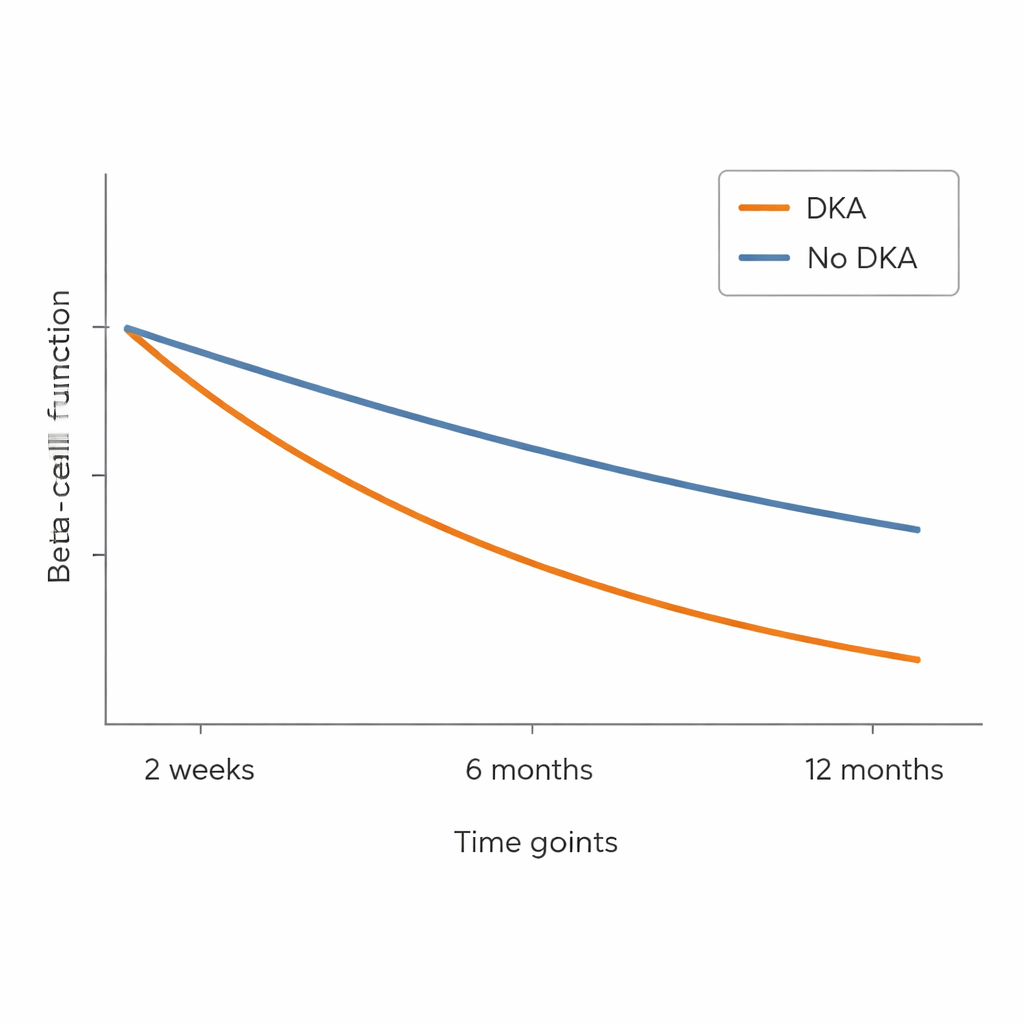
The “honeymoon phase” and what it really shows
Many children with type 1 diabetes go through a “honeymoon phase,” when their insulin needs temporarily drop because their remaining beta cells still produce some insulin. The team looked at this phase using two definitions: a simple threshold of how much injected insulin was needed per kilogram of body weight, and a more refined score that combines insulin dose with HbA1c. By the simpler measure, children with DKA seemed less likely to experience this partial remission. But when the more nuanced combined score was used, the difference between groups largely disappeared. Despite this, the direct biological measure—C‑peptide—still told a clearer story: children who had DKA at diagnosis showed a more pronounced loss of their own insulin production over the year.
What this means for early recognition
For non‑specialists, the study’s message is straightforward: when type 1 diabetes is first recognized before a child becomes critically ill with ketoacidosis, more of the pancreas’s insulin‑producing capacity can be preserved. Children who arrive already in DKA tend to have more injured beta cells, need higher insulin doses to achieve the same blood‑sugar control, and show a faster decline in their own insulin production during the first year. This reinforces the importance of public awareness of early warning signs—such as extreme thirst, frequent urination, weight loss, and fatigue—and of quick medical evaluation. Catching type 1 diabetes before it tips into DKA may help protect the remaining beta cells, easing day‑to‑day management and potentially reducing future complications.
Citation: Niechciał, E., Wais, P. & Kędzia, A. Ketoacidosis at childhood type 1 diabetes onset negatively affects residual beta-cell functions during the first year after diagnosis. Sci Rep 16, 6957 (2026). https://doi.org/10.1038/s41598-026-38533-4
Keywords: type 1 diabetes in children, diabetic ketoacidosis, beta-cell function, C-peptide levels, early diabetes diagnosis