Clear Sky Science · en
High-flow nasal cannula versus noninvasive ventilation in patients with hypoxemic respiratory failure: a prospective cohort study
Breathing Help Without the Tube
When serious lung illness makes it hard to get enough oxygen, many patients land in the intensive care unit. Doctors then face a crucial choice: how to support breathing without immediately putting a tube into the windpipe. This study from a large Chinese hospital takes a close look at two popular options—high‑flow oxygen delivered through soft nasal prongs and a tighter face‑mask machine—and asks whether one keeps patients off a breathing tube or alive longer than the other.
Two Different Ways to Deliver Oxygen
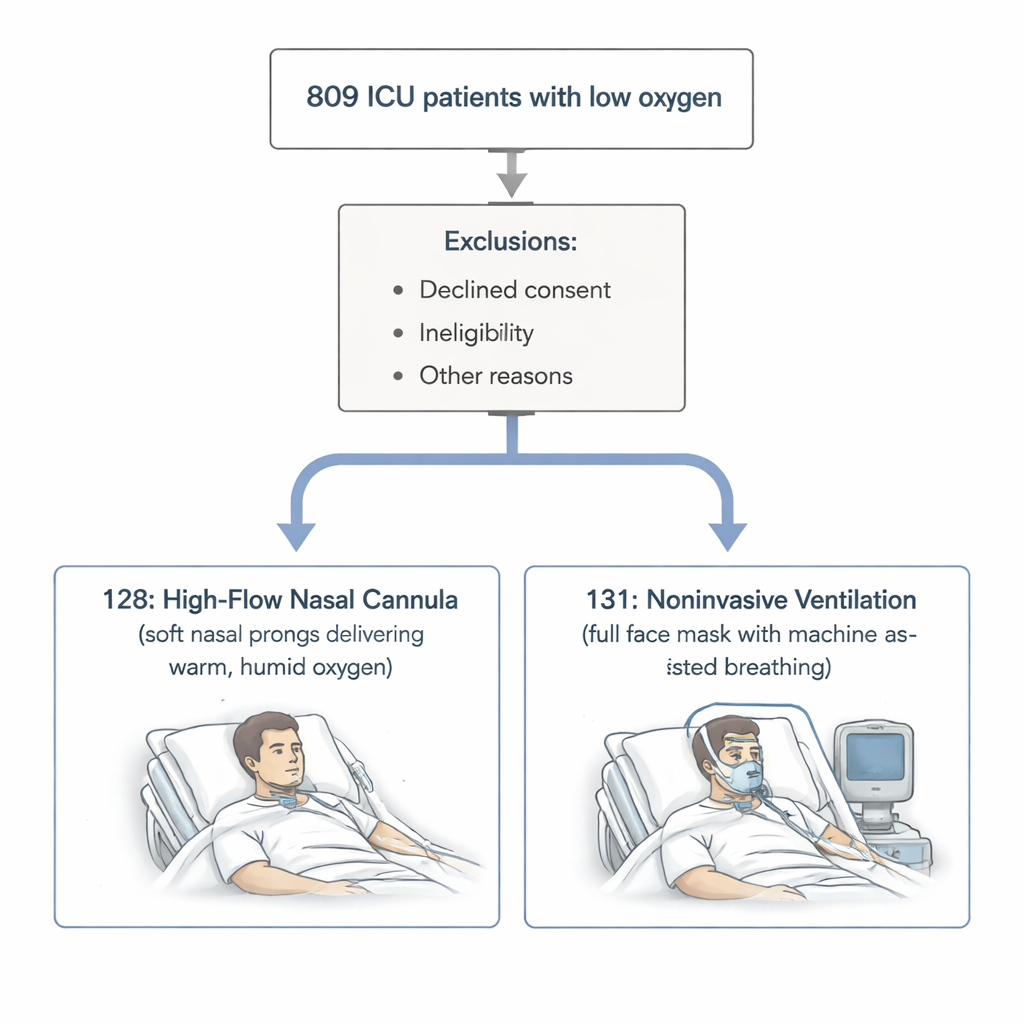
The researchers focused on adults with dangerously low blood oxygen levels but without a buildup of carbon dioxide—people whose lungs struggled to take in oxygen but could still clear waste gas. All were treated in a specialized intensive care unit. One group received high‑flow nasal cannula (HFNC), where warm, humid oxygen is pushed through wide, soft prongs in the nose at high speed. The other group received noninvasive ventilation (NIV), where a machine assists each breath through a sealed face mask. These two methods share the same goals: improve oxygen levels, ease the work of breathing, and avoid the need for a breathing tube placed in the windpipe.
Who Was Studied and What Was Measured
Out of 809 people admitted with low‑oxygen respiratory failure between 2021 and 2023, 259 met strict criteria and agreed to join the study. They were split into 128 patients starting on HFNC and 131 starting on NIV, based on the treating doctor’s judgment. The main yardstick was how many needed to be intubated—that is, placed on an invasive breathing machine—within 28 days. The team also tracked deaths, decisions to stop active treatment, and how long patients stayed in the intensive care unit and in the hospital overall.
Apparent Differences That Faded Under Closer Inspection
At first glance, HFNC looked better. Before any statistical adjustment, fewer HFNC patients needed intubation, and fewer either died or chose to stop active treatment compared with those on NIV. But an important twist emerged: people placed on NIV tended to be sicker at the start, with faster breathing and heart rates. To level the playing field, the researchers used a method called propensity score matching, pairing patients from each group who were similar in age, underlying illnesses, vital signs, and blood‑gas results. Once this matching was done, the early advantages of HFNC disappeared. The two approaches showed no meaningful differences in the chances of intubation, death, combined intubation‑or‑death, or in how long patients spent in the ICU or hospital.
What Happens When the First Choice Fails
The study also examined what happened when HFNC was not enough and treatment had to be “stepped up.” Some of these patients were moved to NIV; others went straight to intubation. Moving from HFNC to NIV did improve oxygen readings, showing that the face‑mask machine can provide stronger support. However, this group stayed in the ICU about four days longer on average than patients who started directly on NIV, raising costs and prolonging intensive care. Despite the longer stay, there was no difference in death rates or total hospital days between those who escalated from HFNC to NIV and those treated with NIV alone. Likewise, among HFNC failures, choosing NIV versus immediate intubation—and the exact timing of that escalation—did not change survival or length of stay.
What This Means for Patients and Families
For people with low‑oxygen respiratory failure but normal carbon dioxide levels, this work suggests that both high‑flow nasal prongs and a noninvasive face‑mask ventilator are reasonable starting options, with similar odds of avoiding a breathing tube and of surviving the hospital stay. NIV may be a better first step in those who are more severely ill or extremely short of breath, because it can shorten time in the ICU, even if it does not change survival. Once high‑flow nasal therapy is clearly failing, however, shifting to NIV or moving directly to intubation appears to make little difference to the final outcome; what matters more is recognizing failure early and acting decisively. Because the study was not randomized and doctors chose treatments based on their clinical judgment, the authors caution that hidden biases may remain and call for large, carefully controlled trials before firm treatment rules are set.
Citation: Qianru, Z., Heyue, J., Longfang, P. et al. High-flow nasal cannula versus noninvasive ventilation in patients with hypoxemic respiratory failure: a prospective cohort study. Sci Rep 16, 6900 (2026). https://doi.org/10.1038/s41598-026-38516-5
Keywords: high-flow nasal cannula, noninvasive ventilation, acute respiratory failure, intubation, ICU care