Clear Sky Science · en
Acute effects of intravitreal aflibercept injections on intraocular pressure in vitrectomized and silicone-oil-filled eyes: a prospective cohort study
Why eye shots matter for everyday vision
Millions of people with diabetes, macular degeneration, or vein blockages in the eye now rely on medicine injected directly into the eyeball to preserve their sight. These quick clinic procedures are highly effective, but they cause a brief jump in pressure inside the eye, and very high pressure can damage the optic nerve. This study asks a practical, anxiety‑provoking question for many patients and clinicians: are these pressure spikes any more dangerous in eyes that have already undergone major surgery and are filled with silicone oil, or had the natural eye gel removed, compared with eyes that were never operated on?
Three kinds of eyes, one kind of treatment
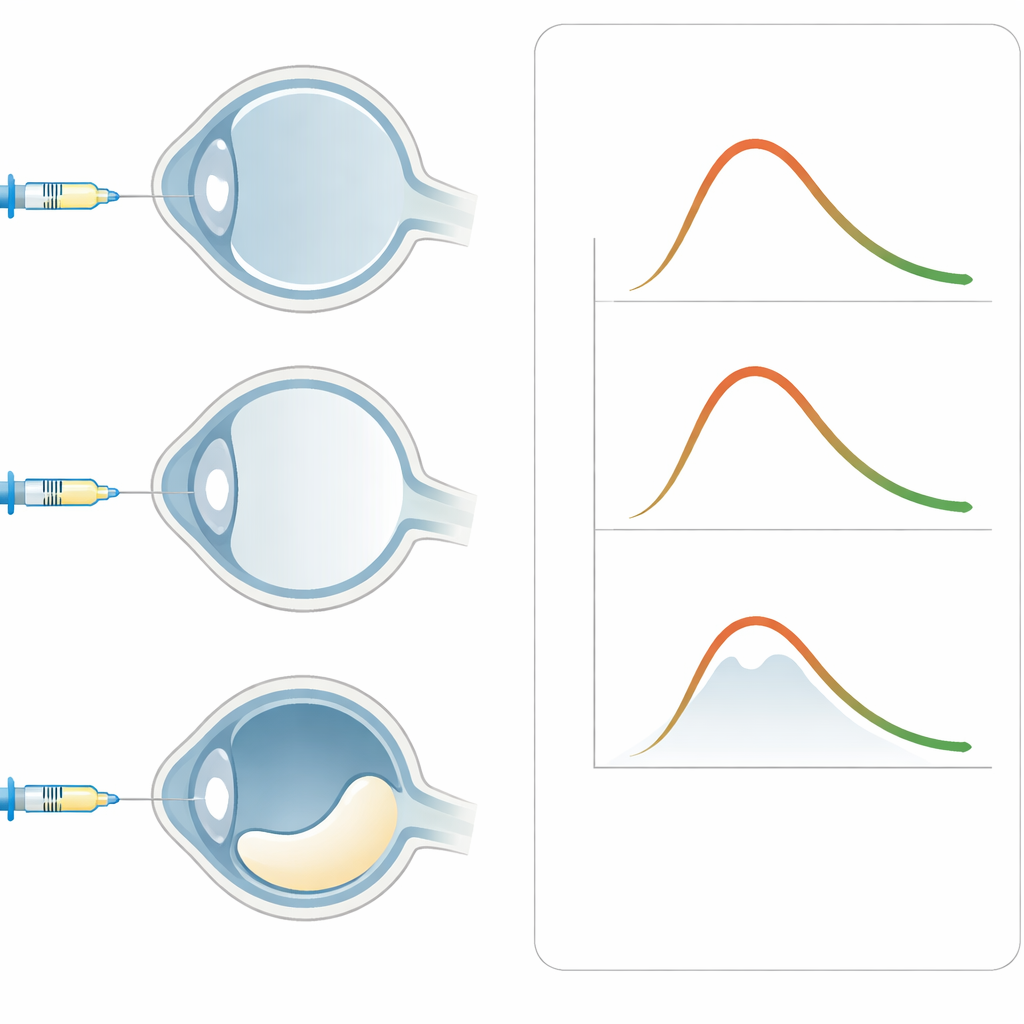
The researchers followed 67 eyes from 58 adults who were scheduled to receive an injection of aflibercept, a commonly used drug for retinal disease. They divided the eyes into three groups based on what filled the back chamber: normal, untouched gel inside the eye; eyes that had previously undergone vitrectomy surgery where this gel was removed; and eyes that had vitrectomy plus a silicone oil fill, often used as an internal bandage after complex retinal repair. Aside from these differences, none of the eyes had glaucoma or were taking pressure‑lowering drops, so the team could focus on how the injection itself affected internal eye pressure.
Watching pressure rise and fall minute by minute
Each eye received a standard dose of aflibercept injected into the back chamber with a fine needle, using a uniform technique to avoid leakage. The team then measured eye pressure just before the injection, within one minute afterward, several times over the next three hours, and again the next day and one week later. They used the classic clinic standard, the Goldmann applanation tonometer, and also a handheld rebound device that does not require numbing drops. This dense series of measurements allowed them to draw detailed curves showing how quickly pressure spiked and then settled down in each type of eye.
Same pressure spike, same recovery in all eye types
Immediately after the injection, pressure inside the eye jumped to about 49 millimeters of mercury in all three groups—roughly three times the typical starting level. Importantly, this surge looked almost identical whether the eye was normal, had its gel removed, or was filled with silicone oil, and no eye lost light perception or needed emergency pressure‑lowering treatment. Over the next three hours, pressure steadily fell back toward baseline in every group, and by three hours it had essentially normalized. Even within the silicone‑oil group, eyes with visible tiny oil droplets near the drainage tissue behaved the same as those without such droplets, suggesting that these short‑term spikes are driven mainly by the simple addition of fluid volume rather than by the eye’s surgical history.
Past injections and pressure gadgets
The investigators also examined whether eyes that had already received several injections in the past reacted differently. Overall, eyes with and without prior injections showed very similar pressure curves, with only a slightly higher reading at one early time point in previously treated eyes—an effect whose real‑world importance remains uncertain. When comparing the two measuring tools, the handheld rebound device agreed fairly well with the Goldmann method at normal or mildly raised pressures, but it became less reliable at the very high levels seen right after injection. It tended to underestimate pressure when it was extremely elevated, which could be critical in people who already have fragile optic nerves.
What this means for patients and clinicians
This work suggests that for the crucial first hours after an aflibercept shot, eyes that have undergone vitrectomy or are filled with silicone oil do not face a special extra risk from pressure spikes compared with untouched eyes. All three groups experience a sharp but brief rise in pressure that settles without intervention in otherwise healthy drainage systems. For routine follow‑up in people without glaucoma, the simpler handheld device may be a convenient way to track these changes, though the traditional Goldmann test remains the safer choice when extremely high pressure or existing optic nerve damage is a concern. In practical terms, the study reassures patients and surgeons that continuing aflibercept treatment after complex retinal surgery can be done without changing the injected volume solely out of fear of short‑term pressure surges.
Citation: Szabó, Á., Thury, G., Baranyi, N. et al. Acute effects of intravitreal aflibercept injections on intraocular pressure in vitrectomized and silicone-oil-filled eyes: a prospective cohort study. Sci Rep 16, 9319 (2026). https://doi.org/10.1038/s41598-026-38455-1
Keywords: intravitreal injection, eye pressure, aflibercept, vitrectomy, silicone oil