Clear Sky Science · en
Anatomic safeguards and the low risk of vascular injury during percutaneous tricortical S1 pedicle screw fixation – a cadaver study
Why screws in the spine don’t usually hurt big blood vessels
Surgeons often stabilize the lowest part of the spine with metal screws, placing them through the back of the pelvis into the first sacral vertebra (S1). Because major blood vessels lie just in front of this bone, it seems these screws should frequently damage them. Yet serious vessel injuries are very rare. This study of donated human bodies set out to understand why, and what natural safeguards in our anatomy help keep patients safe.
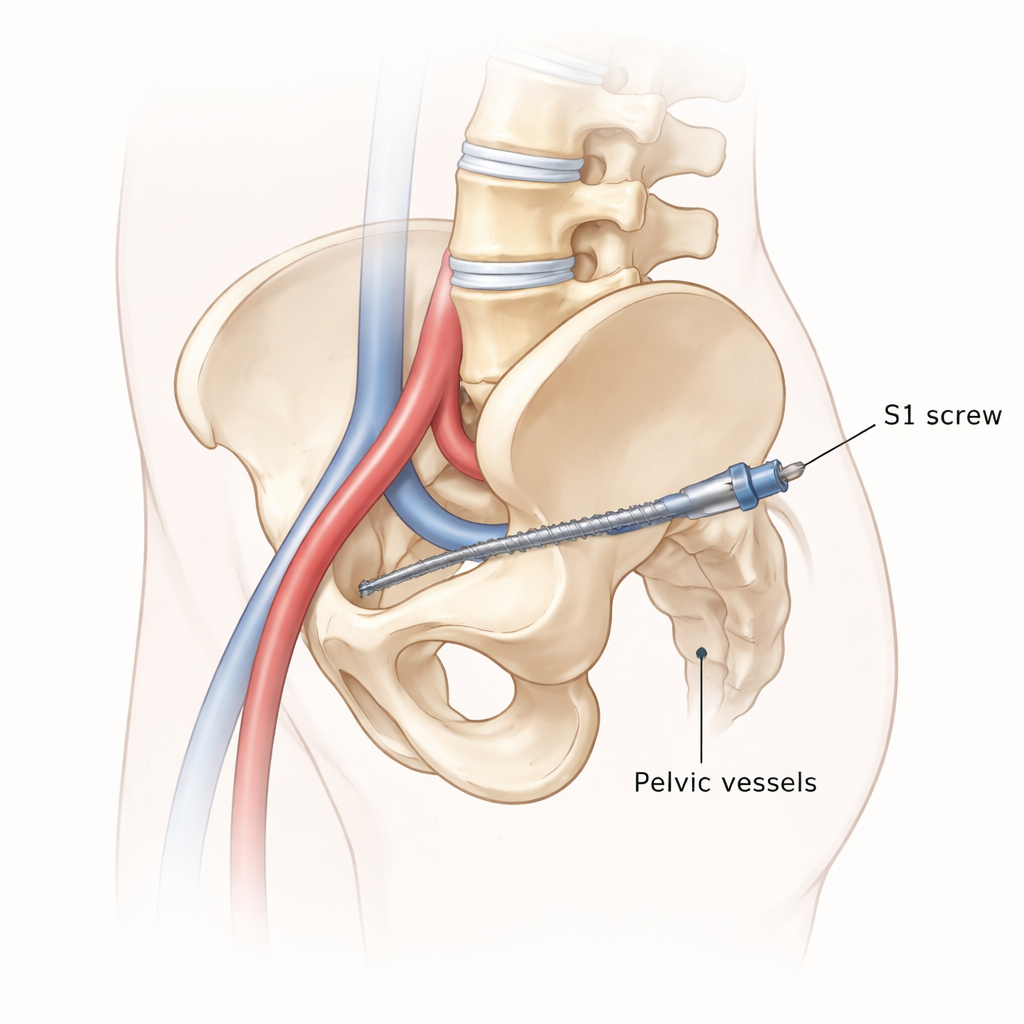
How surgeons anchor screws in the base of the spine
The lowest part of the spine, where the lumbar spine meets the sacrum, carries a great deal of load. To fix instability there, surgeons commonly insert screws through the bony “pedicles” of S1. The strongest method is called tricortical fixation, in which the screw passes through three layers of hard outer bone and its tip ends just beyond the front edge of the sacral “promontory,” the forward‑jutting rim of the sacrum. This gives excellent grip but raises the worry that a screw could pierce nearby blood vessels, especially the common iliac veins and arteries that curve just in front of this area.
A careful experiment using donated bodies
To examine the true risk, the researchers operated on 17 fresh human cadavers, placing a total of 34 screws into S1 using X‑ray guidance similar to modern minimally invasive surgery. They aimed each screw so its tip extended only two threads beyond the front surface of the sacrum. After the screws were in place, most bodies were turned onto their backs and carefully dissected. The team exposed the pelvic organs, the front of the sacrum, and all nearby blood vessels without disturbing their natural relationships, then inspected exactly where the screw tips lay. In some cadavers they also performed three‑dimensional fluoroscopy, a type of CT‑like X‑ray, to measure the angle of the screws and the distance to major vessels.
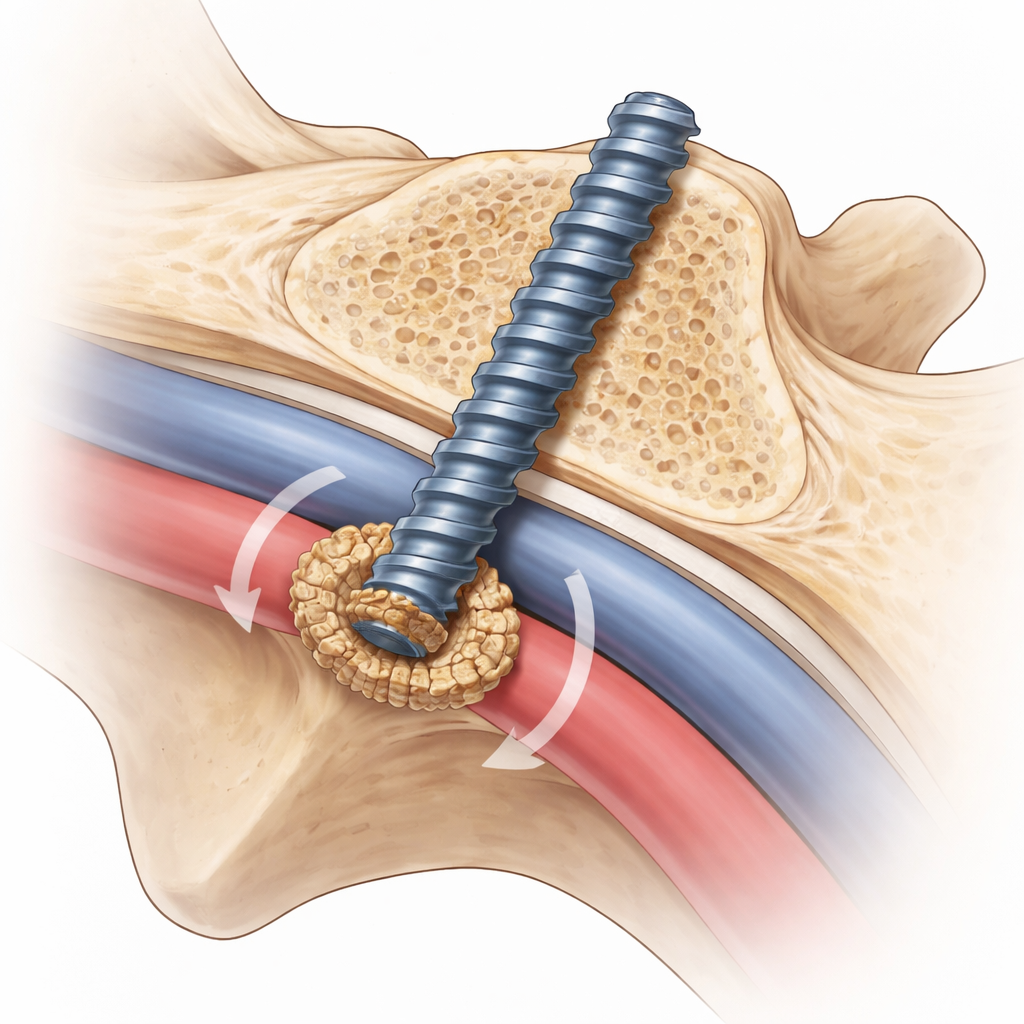
What they found around the screw tips
None of the screws ended up inside a major blood vessel, and no vessel wall was visibly damaged. In two cases out of twelve dissected specimens (about 8%), the screw tip pushed through a tough band of tissue called the anterior longitudinal ligament and came to rest against the outer covering of the right common iliac vein. Even then, the vein was not dented or torn. In another two cases, a screw pointed toward the same vein but was still fully covered by the ligament. In the remaining 84% of cases, the screw tips sat within or behind bony overgrowths called osteophytes on the front of the sacrum. These bony ridges, common in older adults with wear‑and‑tear changes, surrounded the tips and directed them away from the major vessels.
Natural shields and the importance of screw direction
Measurements from 3D imaging showed that screws converged inward at about 19 degrees on average and that the mean distance from screw tips to the iliac vessels was roughly one centimeter. The authors argue that the most important safety factor is not just how far the screw tip extends, but the direction of its path relative to the course of the vessels. When the screw trajectory is aimed toward the center of the sacral promontory, it tends to miss the vessels altogether, even if the tip comes close. The anterior ligament and the ring of osteophytes provide additional buffering, helping prevent direct contact or penetration, although they cannot be seen clearly on the surgeon’s live X‑ray images.
What this means for patients and surgeons
For lay readers and patients, the key message is reassuring: when surgeons follow careful technique—limiting the screw’s length, directing it toward the midpoint of the sacral promontory, and avoiding over‑advancing guide wires—the risk of injuring major pelvic blood vessels appears very low. The body’s own structures, especially age‑related bony overgrowths and strong front ligaments, often act as natural guards in front of the screw tips. While rare delayed problems from long‑term contact with a vessel cannot be completely ruled out, this cadaver study supports the view that modern minimally invasive tricortical screw fixation at S1 is generally a safe and effective way to stabilize the base of the spine.
Citation: Koeck, K., Reissig, L.F., Hainfellner, A. et al. Anatomic safeguards and the low risk of vascular injury during percutaneous tricortical S1 pedicle screw fixation – a cadaver study. Sci Rep 16, 7126 (2026). https://doi.org/10.1038/s41598-026-38331-y
Keywords: spinal fusion, sacral pedicle screws, vascular injury, minimally invasive spine surgery, pelvic anatomy