Clear Sky Science · en
Development of a nomogram to predict in-hospital mortality of trauma patients in the ICU: an analysis of the MIMIC-IV database
Why predicting trauma outcomes matters
Severe injuries from crashes, falls, or violence often land patients in intensive care units, where doctors must make quick decisions with limited information. Families want to know: Will their loved one pull through? This study used a large U.S. hospital database to build a simple bedside tool that helps doctors estimate the risk of dying in the hospital for adult trauma patients in the ICU, using only a handful of routinely measured factors.
Looking for patterns in thousands of ICU cases
To uncover which factors truly matter, the researchers turned to MIMIC-IV, a public database containing detailed records from more than 50,000 ICU stays. From this trove, they identified 2,205 adults admitted with traumatic injuries such as brain trauma, spinal cord damage, chest and abdominal injury, or major fractures. They applied strict criteria to include only first ICU stays, exclude extremely short or unusually long admissions, and remove records missing key information. The patients were then split into two groups: about 70% to build the model and 30% to test whether it worked on new cases. 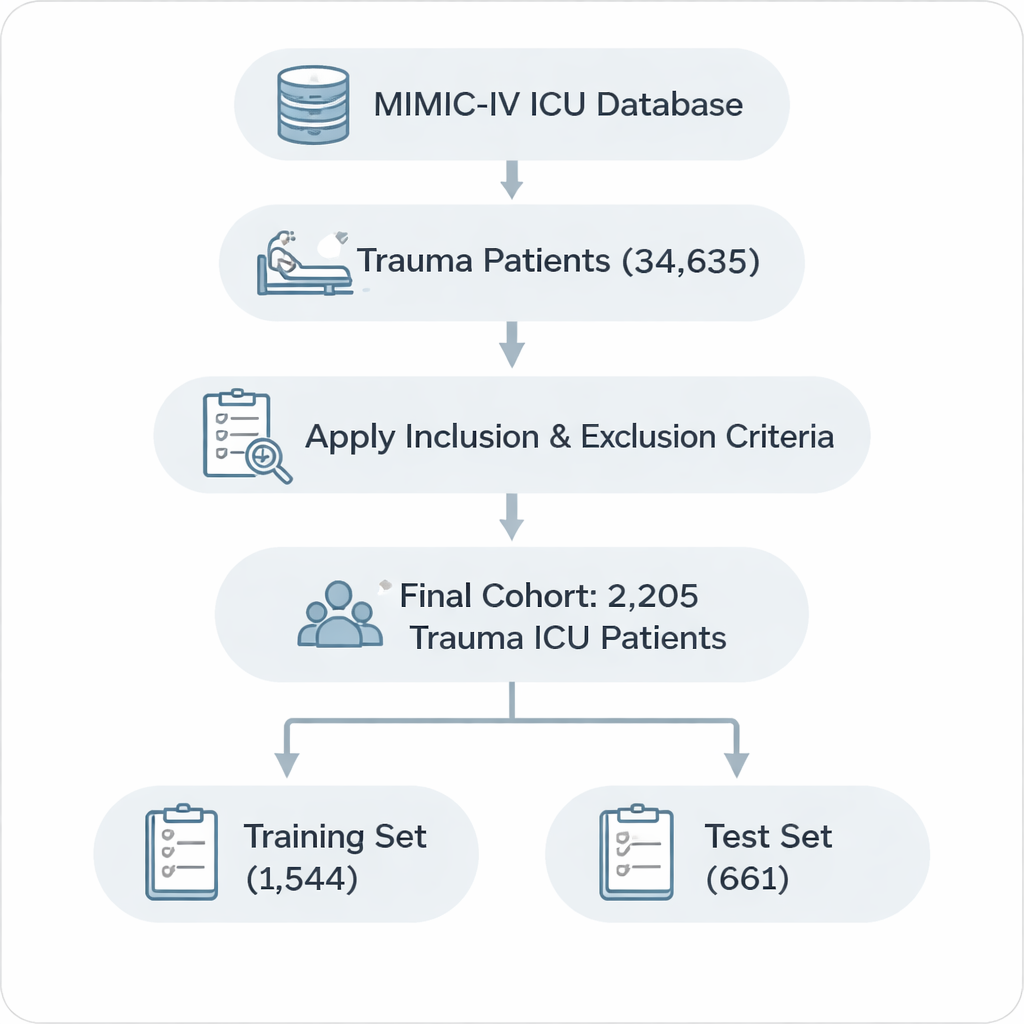
From dozens of measurements to a vital few
Modern ICUs track an enormous volume of data: lab tests, vital signs, existing illnesses, and scores that summarize how sick a patient is. The team began with 49 such indicators measured within the first 24 hours after ICU admission, ranging from blood counts and electrolytes to chronic conditions like heart failure or liver disease. To avoid a confusing, overfitted model, they used a statistical technique called LASSO to shrink and filter this long list down to the most informative predictors. A second, more traditional analysis then checked which of these candidates were independently linked to whether patients survived their hospital stay.
Six everyday measures that tell a powerful story
After this winnowing process, just six factors stood out as core predictors of in-hospital death. Two came from a patient’s medical history: liver disease (hepatopathy), which strongly increased risk, and obesity, which—somewhat surprisingly—was linked to lower risk, echoing an “obesity paradox” seen in other trauma studies. Three were simple lab or bedside measures: the level of chloride in the blood, body temperature, and the white blood cell count, which reflects inflammation and possible infection. The final factor was Acute Physiology Score III (APS III), a composite score that captures how severely ill a patient is overall; in this study, it had the largest influence on predicted risk.
Turning statistics into a practical bedside tool
To make these findings usable, the team built a nomogram—a visual ruler doctors can use to add up points for each of the six factors and read off a patient’s estimated chance of dying in the hospital. They then checked how well this tool matched reality. In both the development and testing groups, the model’s predictions lined up closely with actual outcomes, and its accuracy exceeded common benchmarks used in medicine. Additional analyses showed that using this six-factor tool would offer more clinical benefit than relying on any single indicator alone, especially when doctors are trying to identify patients with a moderate risk of death who might benefit from more aggressive care. 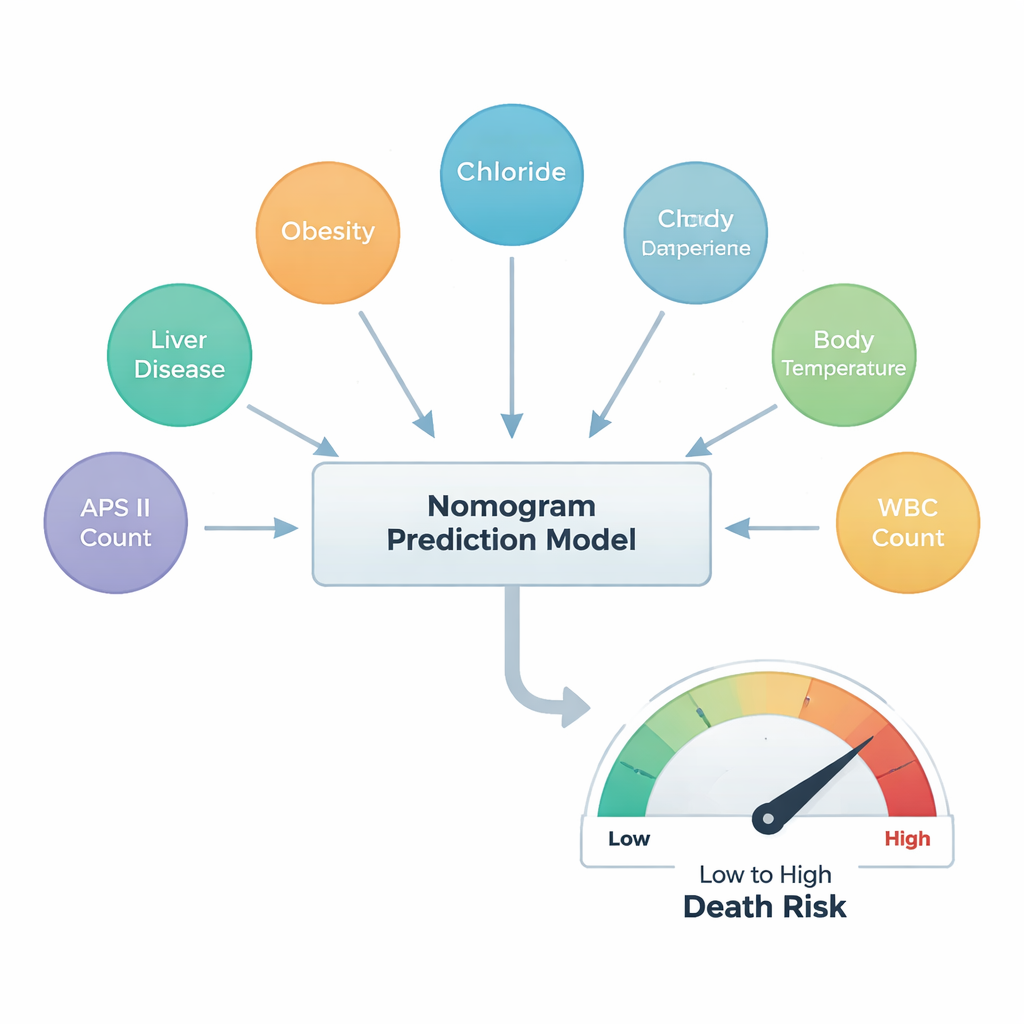
What this means for patients and their families
For people facing severe trauma, no model can guarantee an individual outcome, and the authors stress that their work comes from one hospital system and still needs to be confirmed elsewhere. But this study shows that a short list of familiar ICU measurements—liver disease, obesity, chloride levels, body temperature, white blood cells, and an overall sickness score—can together provide a surprisingly clear picture of survival chances. Used wisely, this simple chart could help ICU teams triage care, communicate more clearly with families, and design future studies to further improve trauma treatment.
Citation: Zeng, Y., Tan, N., He, X. et al. Development of a nomogram to predict in-hospital mortality of trauma patients in the ICU: an analysis of the MIMIC-IV database. Sci Rep 16, 6802 (2026). https://doi.org/10.1038/s41598-026-38251-x
Keywords: trauma ICU, mortality prediction, risk score, critical care, MIMIC-IV