Clear Sky Science · en
Significant ocular residual astigmatism reduces the effect of orthokeratology lenses in controlling myopia
Why this matters for kids who are getting more nearsighted
More and more children around the world are becoming nearsighted, which means their eyes grow too long and distant objects look blurry. Parents and doctors are turning to special overnight contact lenses, called orthokeratology or “ortho-k,” to slow this eye growth. This study asks an important question: do these lenses work equally well for every child, or does the natural shape of the eye make a big difference in how much they help?
How night lenses are supposed to help
Ortho-k lenses are worn during sleep and gently reshape the clear front surface of the eye, the cornea. By morning, many children can see clearly without glasses or contacts, and earlier research suggests that this temporary reshaping can slow how quickly the eye lengthens over time. Slower eye growth is crucial because a longer eye is linked to higher levels of myopia and a greater risk of serious eye diseases in adulthood, such as retinal detachment or glaucoma. But not every child wearing these lenses gets the same level of protection against eye growth, and the reasons have not been fully understood.
A hidden twist in how the eye bends light
Vision is shaped not only by the cornea, but also by hidden structures inside the eye, such as the lens and the back surface of the cornea. Together, these internal parts can introduce a subtle twist or unevenness in how light is focused, known here as ocular residual astigmatism. In everyday life this hidden distortion is partly balanced by the front surface of the cornea, so many children still see reasonably well. However, when ortho-k lenses reshape the front of the eye, that balance is disturbed. The researchers suspected that if a child starts out with a larger amount of this hidden astigmatism, the reshaping from ortho-k might actually uncover more focusing problems and weaken the treatment’s ability to slow eye growth.
What the researchers did and what they found
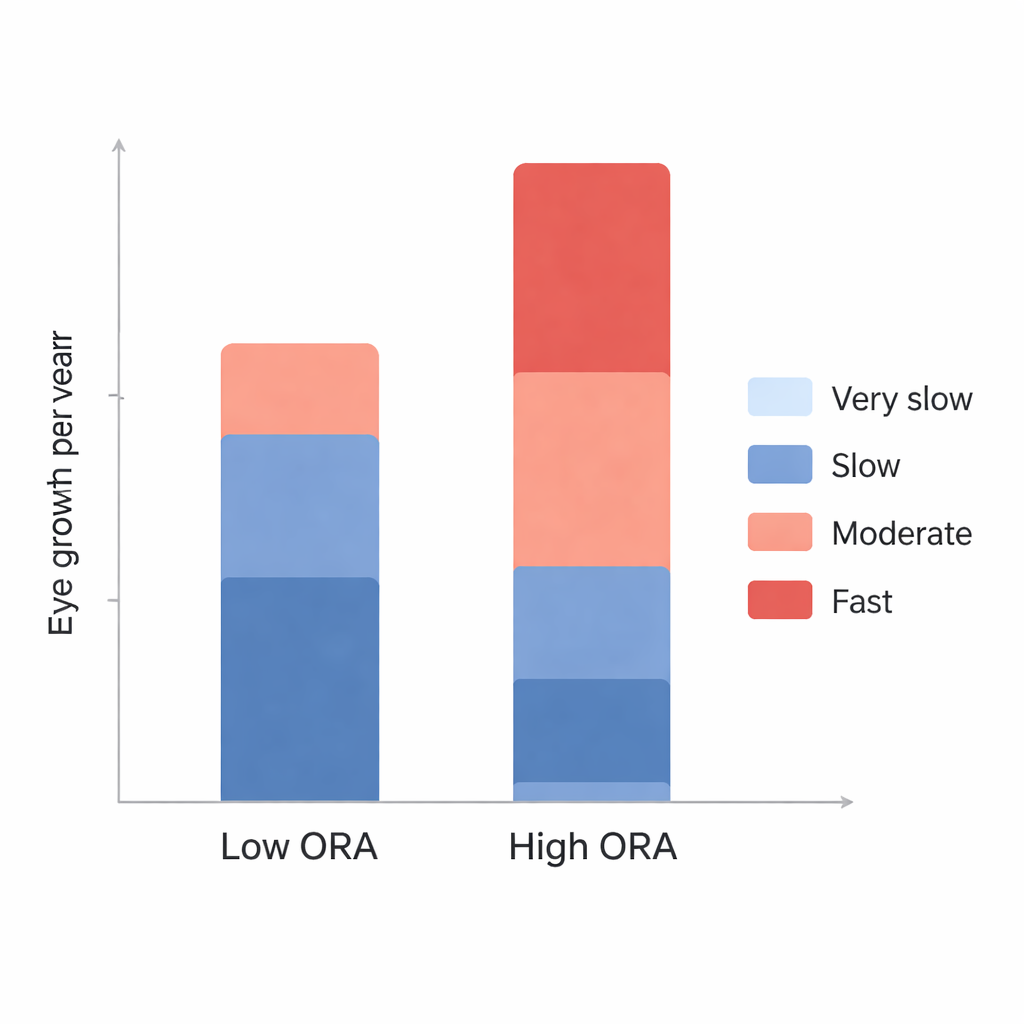
The team examined medical records from 60 children aged 7 to 12 who wore the same brand of spherical ortho-k lenses for one year. All had mild to moderate myopia. The children were divided into two groups based on how much hidden astigmatism they had at the start: a high group (at least 1 diopter) and a low group (less than 1 diopter). The researchers measured the length of the eye several times over the year and calculated how much it grew. Even after accounting for differences in the cornea, they found that eyes in the high hidden-astigmatism group consistently grew more than those in the low group, especially after the first month. By one year, the high group showed roughly twice as much eye lengthening as the low group.
Different growth patterns and who is at higher risk
When the team looked at growth patterns, the contrast was even clearer. In the low hidden-astigmatism group, about one-third of children had very slow eye growth, and a few even showed a slight shortening in eye length. In the high group, almost none had very slow growth, and nearly three-quarters had faster-than-average growth despite wearing ortho-k lenses. A statistical model confirmed that larger hidden astigmatism and stronger starting myopia both predicted more eye growth, while older age predicted less. This suggests that some children, based on the way their eyes focus light internally, are simply less likely to benefit from standard ortho-k designs in terms of slowing myopia progression.
What this means for parents and eye care
For families considering ortho-k lenses, this research highlights that a careful pre-treatment eye exam should include measuring hidden astigmatism, not just the usual glasses prescription and corneal shape. Children with a high level of this hidden distortion may experience less myopia control from standard spherical ortho-k lenses, even if their daytime vision looks sharp. For them, other options such as specially designed soft contact lenses that create beneficial focus patterns across the retina may be a better first choice. Overall, the study supports a more personalized approach to myopia care: rather than assuming that one treatment fits all, doctors can use detailed measurements of each child’s eye to select the strategy most likely to slow their myopia safely and effectively.
Citation: Lin, J., An, D., Lu, Y. et al. Significant ocular residual astigmatism reduces the effect of orthokeratology lenses in controlling myopia. Sci Rep 16, 7319 (2026). https://doi.org/10.1038/s41598-026-38248-6
Keywords: myopia in children, orthokeratology, astigmatism, eye growth, contact lens treatment