Clear Sky Science · en
Polygenic risk score from steroid-sensitive nephrotic syndrome GWAS indicates overlapping genetic basis with steroid-resistant cases
Why children’s kidney diseases share hidden roots
When a child suddenly develops very puffy eyes, swollen legs, and foamy urine, doctors may diagnose nephrotic syndrome, a kidney disorder that leaks too much protein into the urine. Some children improve quickly with steroid medicines, while others do not and face tougher treatments and long‑term problems. This study asks a simple but important question: even though these two groups of children respond differently to drugs, do they share some of the same inherited risk factors deep in their DNA?
Two faces of the same illness
Doctors divide childhood idiopathic nephrotic syndrome into steroid‑sensitive (SSNS), where standard steroid pills bring the illness under control, and steroid‑resistant (SRNS), where they do not. SRNS often leads to more serious kidney damage, transplant, or lifelong treatment. For years, research has shown that many SRNS cases are caused by single, rare gene defects that directly damage key kidney cells called podocytes. SSNS, by contrast, has looked more mysterious, with no single “smoking gun” gene. Instead, large genetic studies across thousands of people have suggested that many small genetic differences, each with tiny effects, combine to raise a child’s risk. This patchwork of small effects is known as polygenic risk.
Measuring inherited risk with a single score
To explore whether SSNS and SRNS might share this kind of polygenic background, the researchers built a polygenic risk score, or PRS. Rather than hunting for one faulty gene, a PRS adds up the influence of hundreds of thousands of common genetic variants, weighted by how strongly they were linked to SSNS in a previous international study of more than 38,000 people. The team then applied this SSNS‑based score to a new group of Chinese children: 493 with SSNS, 123 with SRNS, and 2,506 healthy volunteers. After careful genetic quality checks to ensure everyone in the study shared similar ancestry and that the DNA data were reliable, they compared how high or low the scores were across the three groups. 
A genetic gradient across patient groups
The pattern that emerged was striking. On average, children with SSNS had the highest polygenic scores, clearly higher than those of healthy participants. Children with SRNS had scores that fell in between: lower than SSNS, but still noticeably higher than healthy controls. Statistical tests confirmed that these differences were extremely unlikely to be due to chance. In other words, the same bundles of common genetic variants that help nudge a child toward steroid‑sensitive disease appear to be present, though more weakly, in many children whose disease does not respond to steroids. This graded pattern across healthy children, SRNS patients, and SSNS patients supports the idea that all three lie along a single spectrum of inherited risk rather than in completely separate categories. 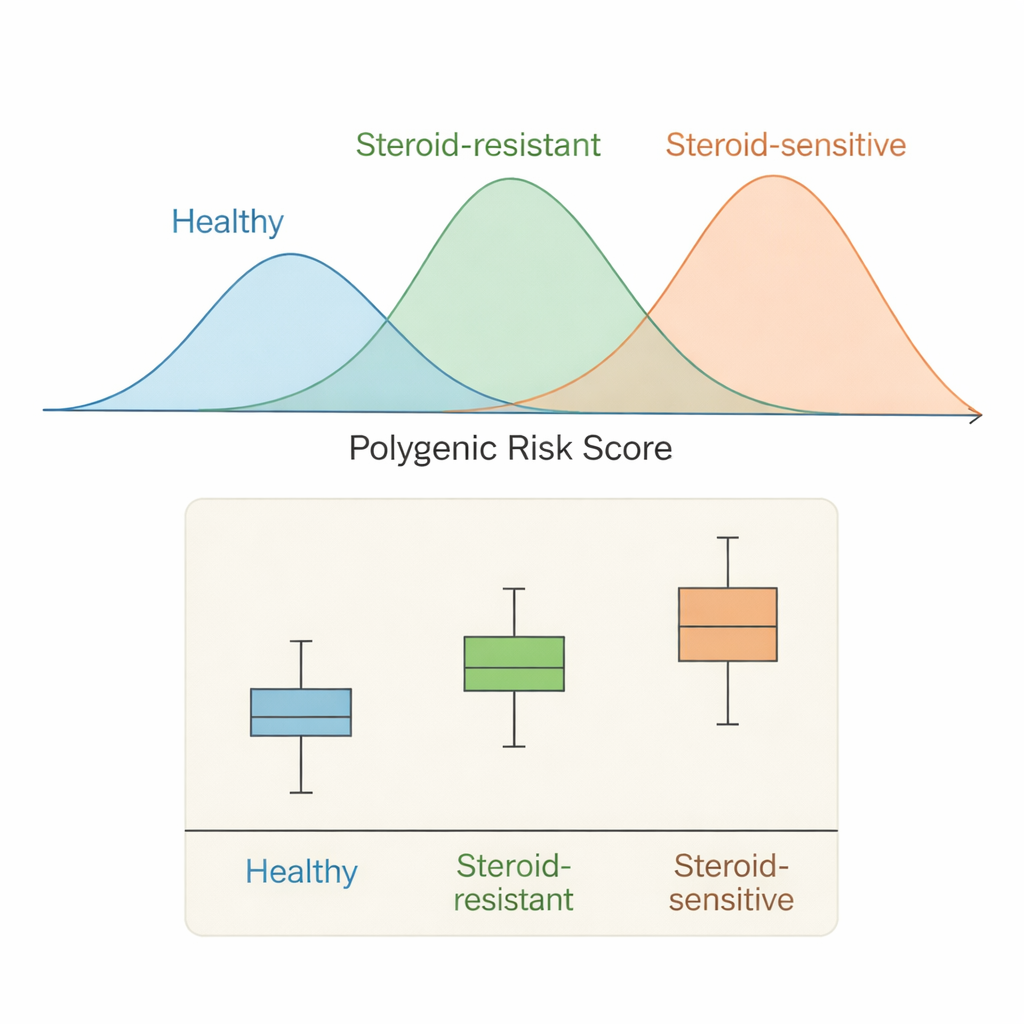
What this means for future care
The findings suggest that SRNS is not explained only by rare, powerful mutations; for many children, a background of many small‑effect variants also contributes. At the same time, the lower scores in SRNS compared with SSNS hint that different biological pathways may dominate in each condition—perhaps more immune‑related influences in SSNS, and a mix of structural and immune factors in SRNS. The authors note important caveats: their SRNS group was relatively small, they could not fully screen for all rare gene defects, and their risk score was built from combined data across many ancestries rather than from East Asian‑specific results. Still, the overall pattern was robust across different checks.
Bringing genetics into the clinic
For families and clinicians, this work does not yet provide a test that can predict exactly which child will respond to steroids. Instead, it offers a clearer picture of how common inherited differences shape risk for both forms of childhood nephrotic syndrome. Over time, as larger studies add more diverse patients and combine information on both rare and common variants, polygenic scores could help doctors identify children at higher genetic risk, tailor follow‑up and treatment intensity, and design trials that match therapies to underlying biology. This study marks a step toward that future by revealing that steroid‑sensitive and steroid‑resistant nephrotic syndromes, though clinically distinct, share important genetic roots.
Citation: Wang, C., Yin, G., Zhou, Y. et al. Polygenic risk score from steroid-sensitive nephrotic syndrome GWAS indicates overlapping genetic basis with steroid-resistant cases. Sci Rep 16, 7141 (2026). https://doi.org/10.1038/s41598-026-38189-0
Keywords: nephrotic syndrome, polygenic risk score, pediatric kidney disease, steroid-resistant nephrotic syndrome, genetic susceptibility