Clear Sky Science · en
Determinants of poor glycemic control in children with type 1 diabetes mellitus in Northwest Ethiopia
Why this matters for families everywhere
For many families, caring for a child with type 1 diabetes means constant attention to food, injections, and blood sugar checks. Yet even with hard work, many children still struggle to keep their blood sugar in a healthy range. This study from Northwest Ethiopia looks closely at why so many kids have poor diabetes control, and how family circumstances and hospital care can make a big difference. Its lessons are relevant not only for Ethiopia, but for any community trying to support children living with this lifelong condition.
A closer look at children living with diabetes
The researchers followed 206 children and teenagers under 18 years old who receive regular diabetes care at two large public hospitals in the city of Bahir Dar. Most of the young patients were around 11 years old, and just over half were girls. The children came from both urban and rural homes, and many families faced economic and educational challenges: nearly one third of caregivers had never been to school, and a large share worked in farming or other low-income jobs. These background details matter because caring for a child with type 1 diabetes requires time, knowledge, and steady access to medicine and food.
How the study measured blood sugar control
Instead of relying on a single blood sugar reading, the team used a test called HbA1c, which reflects average blood sugar over the past two to three months. In countries with fewer resources, experts generally consider an HbA1c level of 7.5 percent or lower to be acceptable for children. Any value above that was labeled as "poor control" in this study. The researchers also gathered information on who cared for the child day to day, whether the family had a home blood sugar meter, how insulin was used and stored, and whether the child had been admitted to the hospital in the previous six months.
What the researchers found
The results were stark: about three out of every four children in the study had poor blood sugar control, with an average HbA1c of 9.2 percent. This level greatly increases the risk of serious short-term problems like diabetic coma, as well as long-term damage to the eyes, kidneys, nerves, and heart. Poor control was common even though all of the children were attending regular clinic visits and had received some form of diabetes education. Many families lacked tools for daily management; for example, only about one quarter had a home glucose meter, and nearly one in four children had missed at least one insulin dose in the week before the survey.
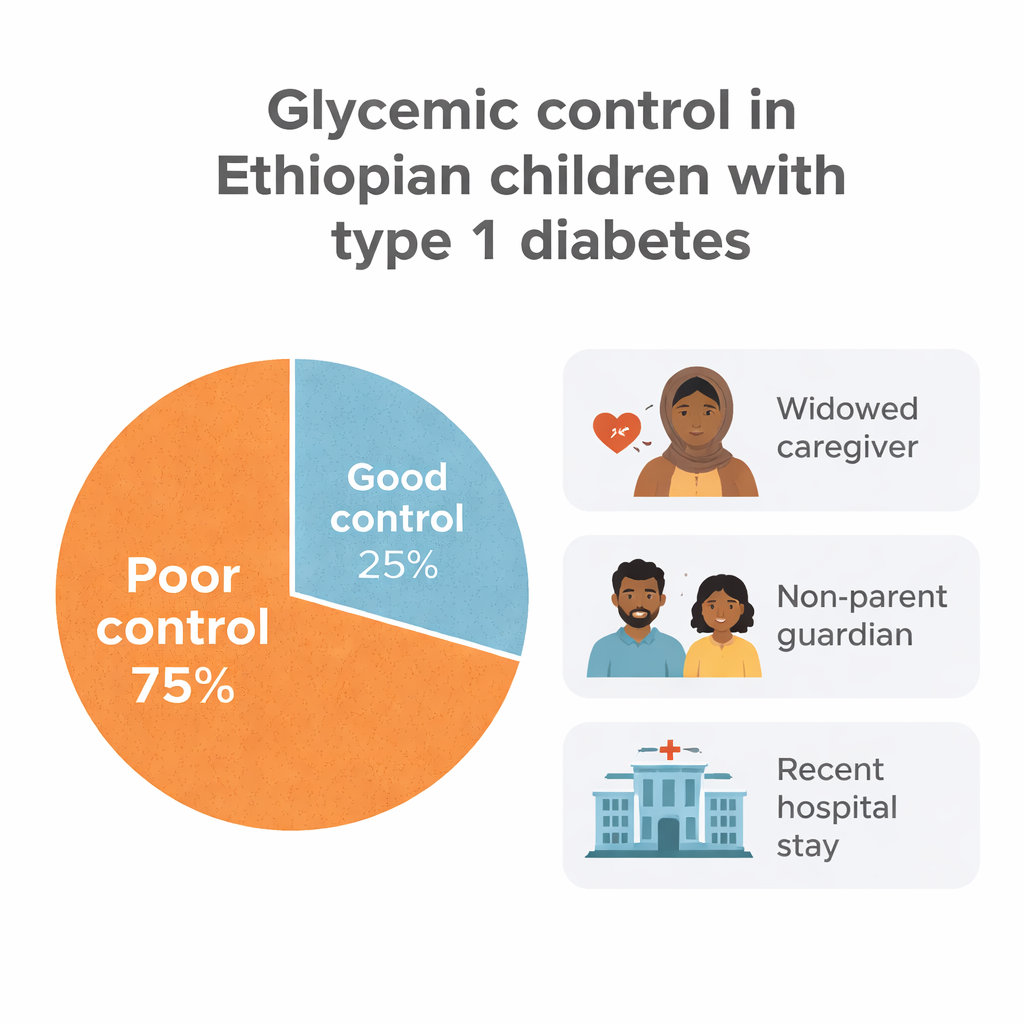
Family structure and recent illness as key warning signs
When the researchers looked more closely at which children were doing worst, family structure stood out. Children whose primary caregiver was widowed, divorced, or single were far more likely to have poor blood sugar control than those with married caregivers. Likewise, when the main caregiver was someone other than the mother—such as a father or another guardian—the child’s control tended to be worse. These patterns suggest that emotional strain, loss of support, and competing demands on caregivers can make the day-to-day routines of diabetes care much harder to maintain. In addition, children who had been admitted to the hospital in the previous six months were much more likely to have poor control, reinforcing the idea that repeated illness and unstable blood sugar go hand in hand.
What this means for care and policy
The study points to practical steps that health systems and communities can take. Clinics need to focus not only on insulin prescriptions, but also on the social realities of the families they serve. Extra attention and support for children living with widowed, divorced, single, or non-parent caregivers could help catch problems early. Regular, easy-to-understand education sessions, better access to HbA1c testing, and follow-up after any hospital admission may prevent future crises. Even in settings where advanced devices are rare, strengthening relationships between health workers, caregivers, and children can improve daily diabetes management and, ultimately, protect young lives.
Citation: Dagne, T.K., Guadie, A.A., Yimer, Y.A. et al. Determinants of poor glycemic control in children with type 1 diabetes mellitus in Northwest Ethiopia. Sci Rep 16, 6811 (2026). https://doi.org/10.1038/s41598-026-38046-0
Keywords: type 1 diabetes in children, glycemic control, caregivers and chronic illness, Ethiopia child health, pediatric diabetes complications