Clear Sky Science · en
Fontan associated protein-losing enteropathy is linked to distinct metabolic and hepatic alterations
Why this rare heart condition matters
The Fontan operation has allowed many children born with only one working heart chamber to survive into adolescence and adulthood. But this life-saving circulation comes at a cost: over time, some patients develop protein-losing enteropathy (PLE), a serious condition where vital blood proteins leak into the gut. This study looks under the hood of the body’s chemistry in children and teens with Fontan circulation, asking how PLE changes their metabolism, liver function, and hormone balance—and whether those changes might one day help doctors detect and manage the problem earlier.
A life with a rerouted heart
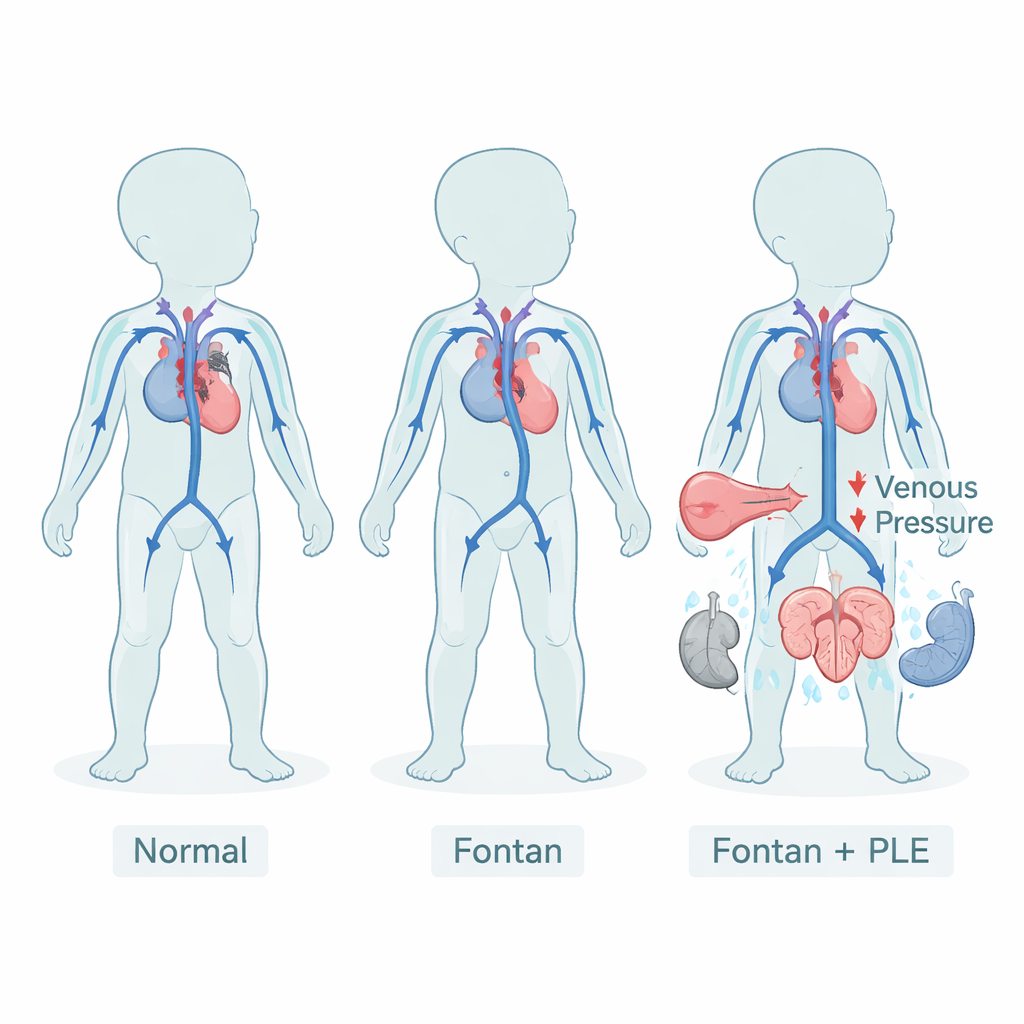
In a normal heart, one pumping chamber sends blood to the lungs and the other sends it to the rest of the body. After a Fontan operation, children born with a single usable ventricle depend on a rerouted circulation: blood returning from the body flows directly into the lungs without a pumping chamber in between. This unusual setup keeps oxygen levels acceptable but requires permanently higher pressure in the veins. Over years, that pressure can strain many organs, including the liver, kidneys, and lymphatic system. One feared consequence is PLE, where proteins that should remain in the bloodstream escape through the intestinal wall, causing swelling, fluid buildup, and vulnerability to infections.
Who was studied and how
The researchers enrolled 49 young people in three groups: 30 with Fontan circulation but no PLE, 10 Fontan patients with diagnosed PLE, and 9 controls who had standard two-ventricle hearts repaired for another defect. All provided blood and urine samples during routine care. The team applied “targeted metabolomics,” a technology that measures many small molecules in the blood at once, including fats, amino acids, bile acids, and signaling chemicals. They combined these detailed profiles with standard lab tests and used statistical models to compare patterns among the three groups, looking for signatures that were specific to PLE rather than to Fontan circulation in general.
Proteins, fats, and a stressed hormone system
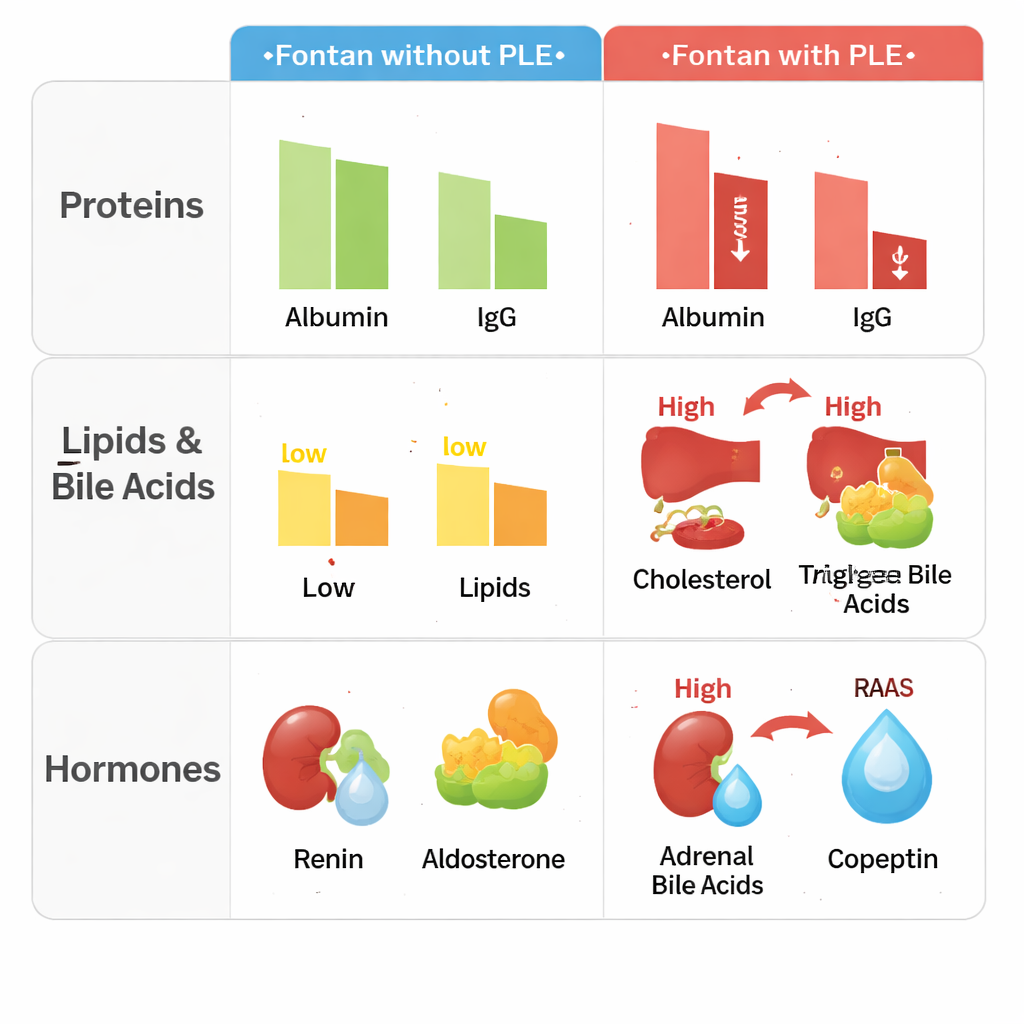
Fontan patients with PLE showed striking losses of blood proteins. Levels of total protein, albumin (which helps keep fluid inside blood vessels), and protective antibodies such as IgG and IgA were all clearly lower than in Fontan patients without PLE or in controls. At the same time, their bodies appeared to be under hormonal stress. Substances that regulate blood pressure and salt balance—renin, aldosterone, and copeptin (a stand-in marker for the hormone vasopressin)—were much higher in PLE patients, suggesting that the kidneys and brain were working hard to conserve salt and water. This pattern fits with the clinical picture of swelling, low blood volume, and circulatory fragility seen in advanced Fontan failure.
Liver signals, altered fats, and bile acids
The study also uncovered a distinctive fingerprint in fats and liver-related chemicals. Compared with healthy controls, Fontan patients without PLE tended to have lower cholesterol, triglycerides, and several phosphatidylcholines, a class of fat molecules important for cell membranes and lipoproteins. Surprisingly, patients with PLE reversed this pattern: many of these lipids, including cholesterol and triglycerides, were higher, forming a gradient from lowest in Fontan without PLE to highest in Fontan with PLE. Markers related to liver cell stress, especially gamma‑glutamyltransferase (GGT), were more abnormal in PLE patients. Certain bile acids—detergent-like molecules made by the liver that also act as chemical messengers—were lower in PLE and showed specific links to both kidney hormones and fat molecules. Together, these changes suggest that PLE is tied not only to leaking proteins in the gut but also to a broader disturbance in how the liver handles fats and bile.
Toward simple blood-based markers
To explore whether combinations of routine tests might flag PLE, the team tested many ratios between proteins, fats, and hormones. Two stood out as especially promising in this small group: the ratio of IgG to aldosterone, and the ratio of albumin to one phosphatidylcholine species (called PC ae C40:3). In PLE patients, these ratios were much lower, reflecting the combination of protein loss and hormone or lipid changes. Even after adjusting for differences in body size, sex, and use of water pills, group status (PLE vs. no PLE) remained the main driver of these ratios. The authors emphasize that these are not ready-made diagnostic tests; they were identified and evaluated in the same small dataset, so their performance may look better than it truly is. Larger, independent studies will be needed before such markers could guide care.
What this means for patients and families
For families living with Fontan circulation, this work underscores that PLE is a whole-body problem, not just a leaky gut. Children with PLE show a coordinated shift in proteins, fats, bile acids, and stress hormones that reflects the combined strain on the heart, liver, kidneys, and lymphatic system. While the study does not yet offer a cure, it maps out new chemical clues that could eventually help doctors detect PLE earlier, monitor its severity, and perhaps target therapies more precisely. In simple terms, the research shows that when protein loss appears in Fontan patients, many other hidden systems are already under pressure—and understanding those changes is a key step toward better long-term outcomes.
Citation: Schroeder, C., Fahlbusch, F.B., Cesnjevar, R. et al. Fontan associated protein-losing enteropathy is linked to distinct metabolic and hepatic alterations. Sci Rep 16, 5256 (2026). https://doi.org/10.1038/s41598-026-37974-1
Keywords: Fontan circulation, protein-losing enteropathy, pediatric cardiology, metabolomics, liver and kidney function