Clear Sky Science · en
Intramuscular neural distribution of the vastus lateralis informs effective and safe botulinum neurotoxin injection
Why knee muscle injections matter
Many people live with stubborn pain at the front of the knee or tight, overactive thigh muscles after stroke or other nerve injuries. One treatment, injections of botulinum neurotoxin (the same family of drugs used in wrinkle treatments), can calm an overactive muscle and rebalance how the kneecap moves. But for the drug to work well and safely, doctors must know exactly where the tiny nerves run inside the muscle they are targeting. This study maps those nerves inside one key thigh muscle, the vastus lateralis, and tests a practical way to guide injections using ultrasound.
A closer look at a key thigh muscle
The vastus lateralis is the large muscle along the outer side of the thigh. It helps straighten and stabilize the knee during everyday activities such as walking, running, and squatting. When it fires too strongly compared with its partner on the inner thigh, the vastus medialis, the kneecap can be pulled slightly outward. Over time this imbalance can increase pressure under the kneecap, damage the joint surface, and cause chronic front-of-knee pain. In people with spasticity—overactive muscles after conditions like stroke or cerebral palsy—an overly tight vastus lateralis can also lock the knee into an awkward, painful position and disrupt walking.
Why the exact nerve map is important
Botulinum neurotoxin works by blocking the chemical signal that nerves use to tell muscle fibers to contract. The effect is strongest when the drug is placed near the muscle’s “hot spots” where nerve branches end and connect to many fibers. Earlier work hinted that these nerve-dense areas in the vastus lateralis are near the upper and middle parts of the muscle, but the details were unclear. Because the muscle is wide and thick, missing those zones can waste drug, weaken nearby muscles, or disturb walking. The authors set out to create a fine-grained map of nerve endings and then turn that map into simple surface landmarks and ultrasound instructions that clinicians can follow at the bedside.
Mapping hidden nerves in donated tissue
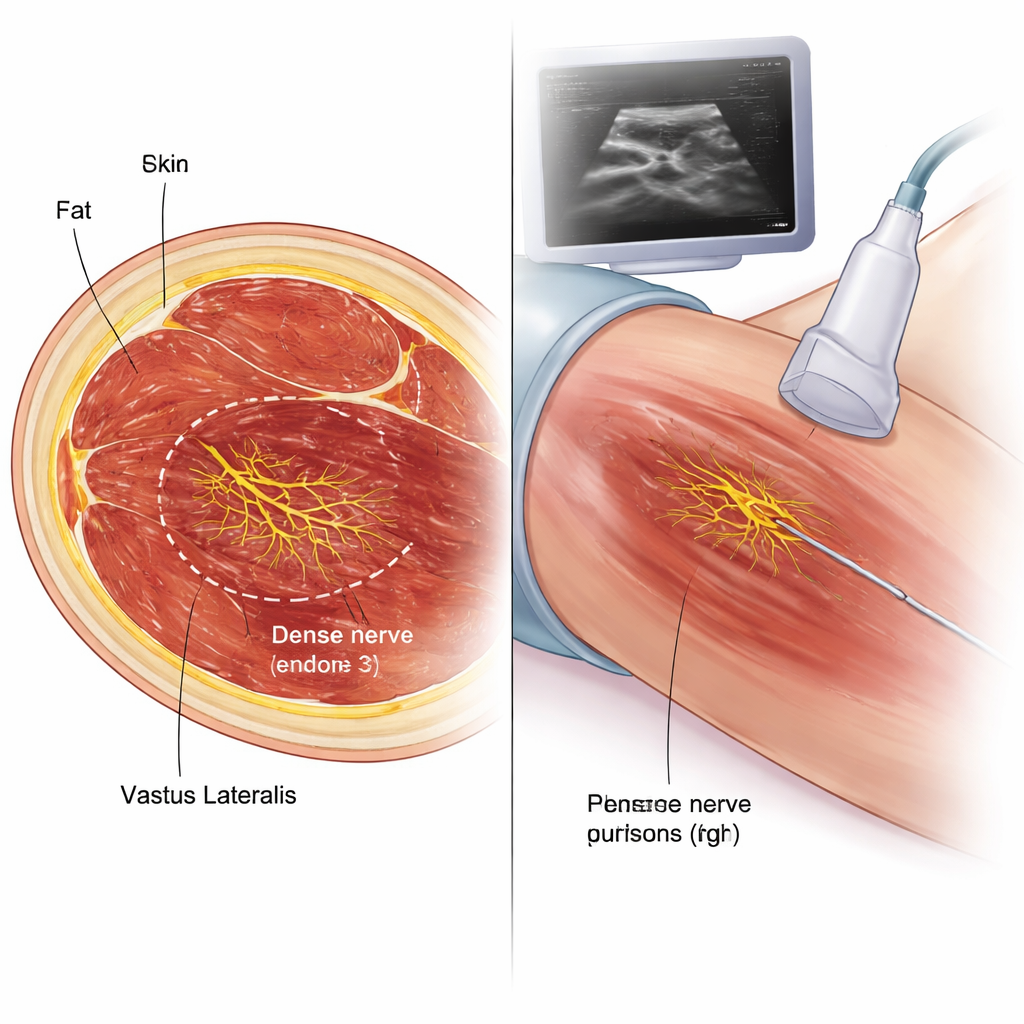
Using 12 donated adult bodies, the researchers carefully exposed the femoral nerve branches that feed the vastus lateralis and recorded where they entered the muscle. They then removed the muscle, divided it into four equal zones from hip to knee, and applied a specialized whole-mount staining technique called Sihler’s method. This process makes the muscle tissue nearly transparent while leaving the nerves darkly stained, allowing the tiny branches and their endings to be traced under low magnification without cutting the tissue into slices. Three observers counted nerve endings in each zone to determine where the muscle’s wiring was densest.
Finding the best target zone and testing it
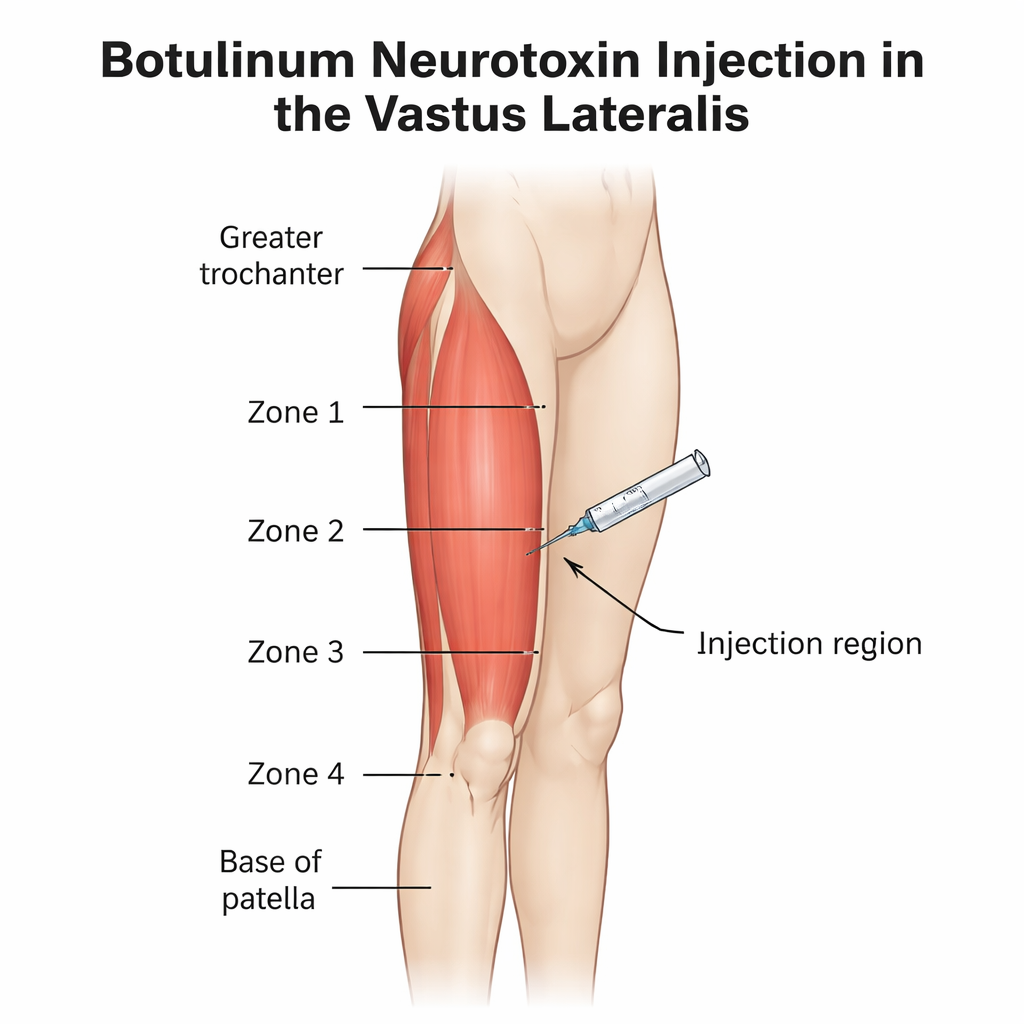
The nerve branches most often entered the vastus lateralis in the upper and middle zones, with no new branches entering at the lowest quarter near the knee. When the team counted endings, they found that the mid-lower quarter—zone 3, roughly between the halfway and three-quarters points from hip to knee—had the highest concentration of nerve endings, about 40% of the total. To turn this into a practical injection guide, they used ultrasound on two fresh cadavers to measure skin, fat, and muscle thickness and to distinguish the vastus lateralis from its neighbors. They marked a line between the bony bump at the side of the hip (greater trochanter) and the base of the kneecap, then chose the midpoint of this line on the outer third of the thigh as the injection site. Under real-time ultrasound, a fine needle was advanced into the thickest part of the vastus lateralis and a small amount of blue dye was injected.
How well the guided injections worked
After these ultrasound-guided injections, the researchers dissected the thighs to see where the dye had gone. Even with only 2 milliliters of fluid, the dye spread along the muscle fibers over about 15 centimeters, covering the main nerve-dense regions in zones 2 to 4 while staying confined inside the vastus lateralis. Importantly, there was no leakage into neighboring muscles and no accidental passage through major nerves or blood vessels. Measurements showed that skin and fat thickness were fairly consistent, while the muscle itself was thickest around zone 3, matching the area of densest nerve endings. This supports the idea that a single, well-placed injection at the mapped site can reach many of the muscle’s key nerve endings without risking damage elsewhere.
What this means for patients
For people with persistent front-of-knee pain or muscle tightness that has not improved with exercise and physical therapy, botulinum neurotoxin injections into the vastus lateralis are an emerging option. This study shows that the middle portion of the outer thigh, around the mid-distance between hip and knee, contains the most nerve endings feeding this muscle. By combining simple body landmarks with ultrasound imaging, clinicians can place injections more accurately, using lower doses while reducing the chance of side effects such as gait disturbance or unwanted weakness in nearby muscles. Although the work was done in older donated bodies and still requires clinical testing in living patients, it provides a clear anatomical blueprint to make these injections safer and more effective.
Citation: Yi, KH., Hu, H., Hwang, SO. et al. Intramuscular neural distribution of the vastus lateralis informs effective and safe botulinum neurotoxin injection. Sci Rep 16, 5353 (2026). https://doi.org/10.1038/s41598-026-37960-7
Keywords: anterior knee pain, vastus lateralis, botulinum toxin injection, ultrasound guided injection, muscle spasticity