Clear Sky Science · en
Application of XGBoost and logistic regression in predicting 90 days mortality for elderly severe acute renal failure patients
Why this research matters to families and patients
Acute kidney failure is a sudden loss of kidney function that often strikes older people in intensive care units. It can turn a serious illness into a life‑threatening crisis, and many families and doctors struggle to know which patients are most at risk of dying in the weeks that follow. This study asks a simple but important question: can modern data‑driven tools help doctors more accurately identify which elderly patients with severe kidney failure are in greatest danger over the next three months, so that care can be better tailored to them?
Who was studied and what the team set out to do
The researchers analyzed records from 7,500 people aged over 60 who were admitted to an intensive care unit in Boston between 2008 and 2019 and developed severe acute kidney failure. About 1,150 of these patients died within 90 days, highlighting just how deadly this condition can be in older adults. Using this large trove of real‑world hospital data, the team compared two ways of turning bedside information—such as age, blood pressure, urine output, and illness‑severity scores—into a prediction of who would be alive three months later.
Two different ways to "read" the data
The first method, logistic regression, is a long‑standing statistical workhorse in medical research. It looks for straight‑line relationships between risk factors and outcomes and is valued because doctors can easily see how each factor, such as age or blood pressure, pushes risk up or down. The second method, called XGBoost, belongs to a newer family of machine‑learning tools. Instead of one straight line, it builds many small decision trees that together can capture complex, curved patterns in the data—for example, where risk rises sharply only after several risk factors line up. Because of this, XGBoost can, in theory, squeeze more predictive power out of the same hospital information, though it is harder to interpret at a glance.
What the models found about risk
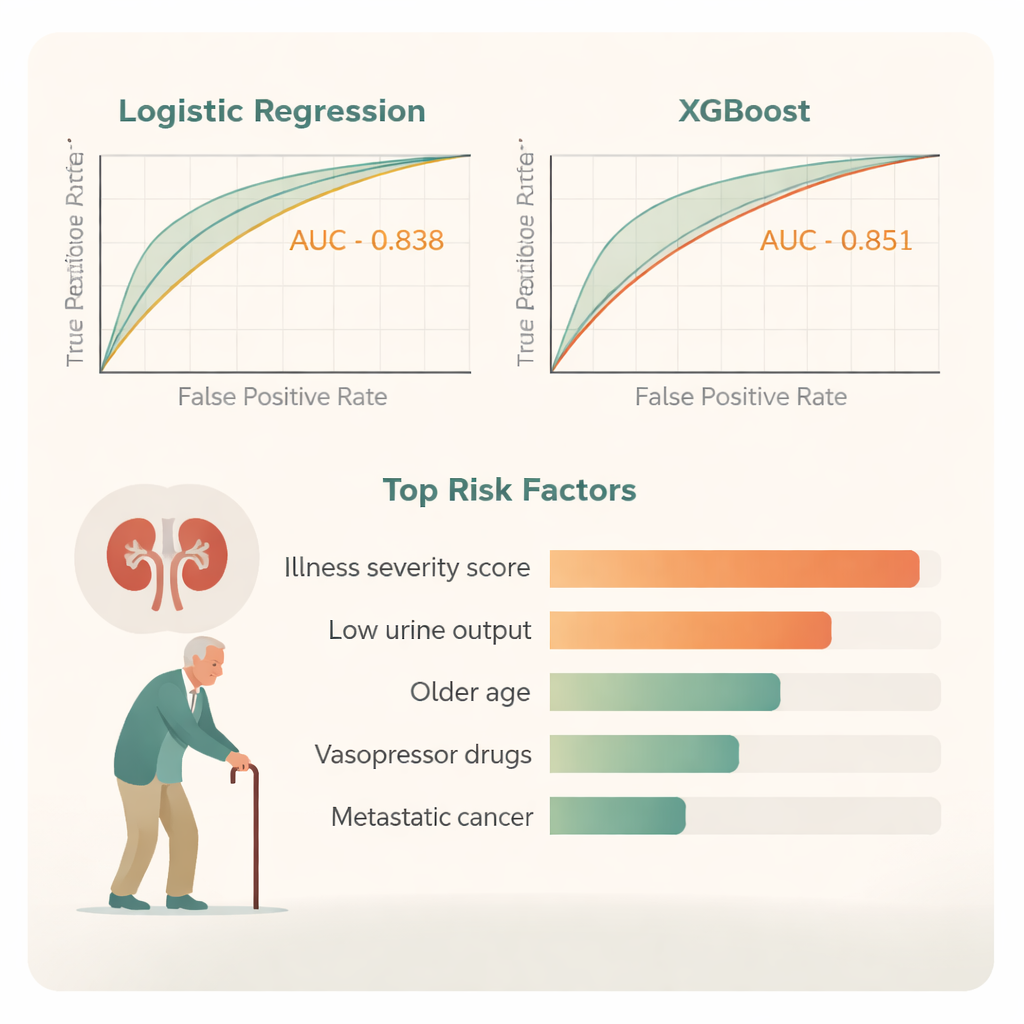
Both approaches were fed the same carefully cleaned data and were tested using strict, repeated cross‑checks to avoid overfitting. Several features consistently stood out as strongly linked to 90‑day death. These included how sick a patient was when they arrived in the ICU (captured by a score called APSIII), how little urine they produced, older age, low blood oxygen levels, and the need for drugs that raise blood pressure, known as vasopressors. Having advanced cancer that had spread to other organs also greatly increased the chance of dying. Together, these factors paint a picture of frailer patients whose bodies are struggling on several fronts at once.
Which prediction method did better
When the two models were compared head‑to‑head, both did a good job of telling apart patients who would survive from those who would not. However, XGBoost performed slightly better: on a standard measure of accuracy called the area under the curve, it scored 0.851, compared with 0.838 for logistic regression. Decision‑curve analysis, a way of judging how useful a model is for real‑life choices such as whether to intensify treatment, showed that XGBoost offered a higher net benefit across a broader range of clinical scenarios. It also produced smaller prediction errors overall. To make this complex model more understandable at the bedside, the team created a “breakdown” plot that shows, for an individual patient, how each factor nudges their predicted risk up or down.
What this could mean for care
For a layperson, the take‑home message is that computers can now help doctors estimate, with reasonable accuracy, which older ICU patients with sudden kidney failure are at greatest risk of dying within three months. In this study, the newer machine‑learning method edged out the traditional approach, especially when many health factors interacted in complicated ways. Still, both tools rely on information that hospitals already collect—such as urine output, age, illness severity, blood pressure and the presence of advanced cancer—and are meant to support, not replace, clinical judgment. If further tested in different hospitals, such models could guide more timely conversations about prognosis, help prioritize scarce intensive‑care resources, and encourage closer monitoring and tailored treatment for those patients whose kidneys, and overall health, are most precarious.
Citation: Zeng, J., Zhu, Y., Ye, F. et al. Application of XGBoost and logistic regression in predicting 90 days mortality for elderly severe acute renal failure patients. Sci Rep 16, 7077 (2026). https://doi.org/10.1038/s41598-026-37828-w
Keywords: acute kidney failure, elderly ICU patients, mortality prediction, machine learning in medicine, logistic regression vs XGBoost