Clear Sky Science · en
High reclassification rate of height-indexed left atrial volume in obese and overweight patients with cardiac pathologies in daily clinical practice
Why the size of a heart chamber matters
For people who are overweight or obese, the way doctors measure the size of one small heart chamber—the left atrium—can change whether they are told their heart is normal or enlarged. That label is important, because an enlarged left atrium is linked to common and serious problems such as irregular heartbeats, stroke, and certain types of heart failure. This study asks a simple but crucial question: are we underestimating how many heavier patients actually have an enlarged left atrium because of how we do the math?
Rethinking a standard heart measurement
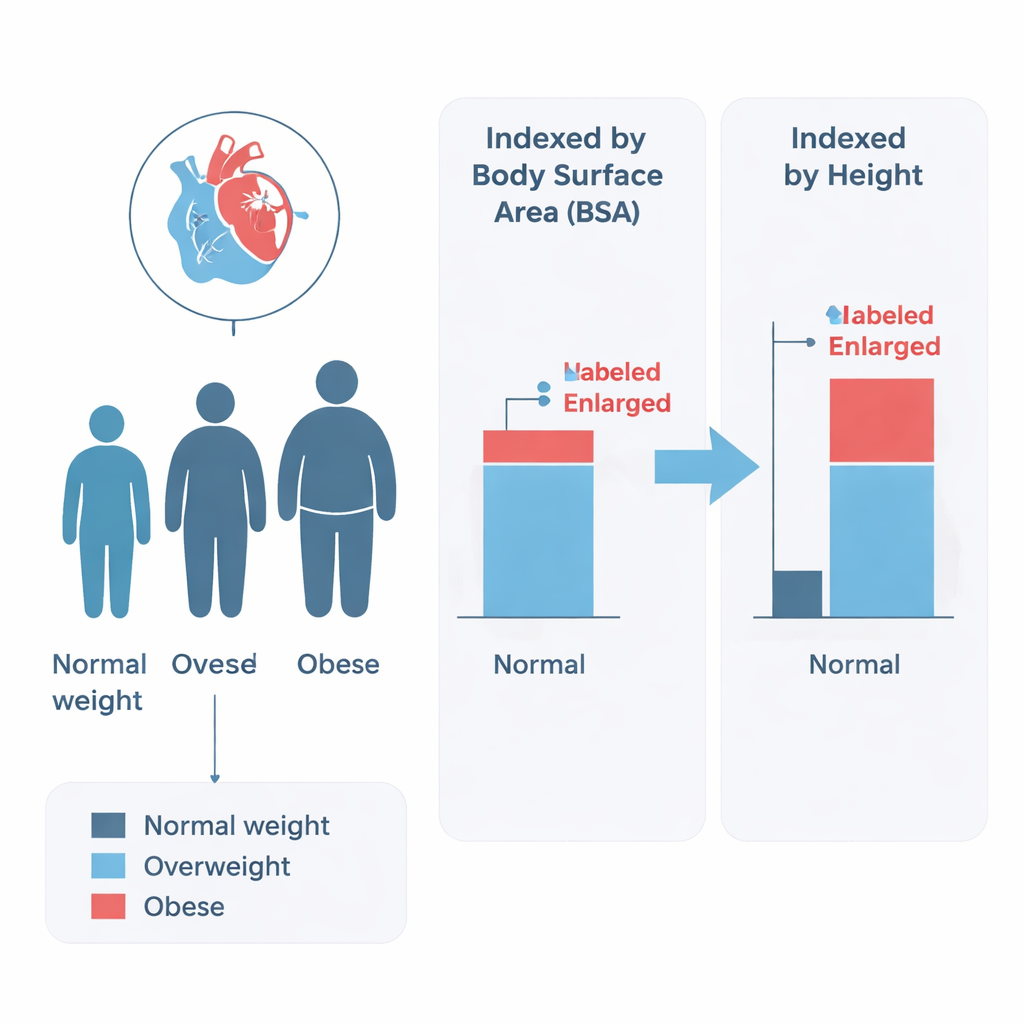
In everyday practice, heart specialists often rely on ultrasound scans (echocardiograms) to check how big the left atrium is. To fairly compare people of different body sizes, they usually “index” the chamber’s volume—that is, divide it by body surface area, which is calculated from weight and height. But in people with obesity, body surface area becomes very large, which can make an already enlarged chamber look deceptively normal after the calculation. The authors wondered whether using a person’s height instead of body surface area would give a more truthful picture of heart strain in heavier patients.
Who was studied and how
The researchers analyzed 253 adults who were already being seen for various heart problems, such as high blood pressure–related heart disease, cardiomyopathy, coronary artery disease, heart failure, and atrial fibrillation. None had major mitral valve disease or completely normal scans. Each person’s left atrial volume was measured by standard ultrasound techniques, and then indexed in three ways: by body surface area, by height, and by height squared. Patients were grouped as normal weight, overweight, or obese based on body mass index. The team then compared how often each person was labeled as having a normal or enlarged left atrium, and how severe that enlargement was, under the different indexing methods.
Hidden enlargement revealed in heavier patients
Across the whole group, about six in ten patients had an enlarged left atrium when the volume was indexed by height, slightly more than when body surface area was used. The differences became striking in people with obesity. Using body surface area, only 46% of obese patients were classified as having an enlarged left atrium. When the same raw volumes were divided by height or height squared, this jumped to about two thirds. Among obese patients whose left atrium looked normal by the traditional method, 40% were reclassified as enlarged when height-based indexing was applied. Overweight patients showed a similar, though smaller, shift: about one in five moved from the “normal” to the “enlarged” category when height was used instead of body surface area.
Not just present, but more severe
The change was not only about detecting enlargement, but also about grading its seriousness. In the obese group, half of the patients moved up by at least one severity level—say, from mild to moderate—and more than a third jumped by two grades when height-based indexing was used. In contrast, normal-weight patients rarely changed category. Statistical analyses showed that obesity, having a body mass index above about 27.5, and atrial fibrillation were the strongest predictors of being reclassified from normal to enlarged when switching from body surface area to height. Age, sex, blood pressure–related heart disease, and pumping strength of the main chamber did not independently explain the change.
What this means for patients and doctors
The study suggests that many overweight and obese patients with heart disease may be falsely reassured that their left atrium is normal when traditional indexing by body surface area is used. Because left atrial enlargement helps diagnose conditions like heart failure with preserved ejection fraction and predicts future events such as stroke and death, missing it could delay treatment or risk assessment. By simply switching to indexing left atrial volume by height (or height squared), clinicians are more likely to uncover early or more advanced enlargement in heavier patients and better match treatment to true risk.
A clearer way to size the heart
To a layperson, the message is straightforward: for people who are overweight or obese, using height instead of body surface area gives a clearer, more honest measurement of a key heart chamber. This study, together with other research, supports the idea that doctors should routinely rely on height-based calculations when judging whether the left atrium is enlarged in heavier patients. Doing so may improve diagnosis, guide therapy more accurately, and ultimately help prevent serious complications linked to a silently overstretched heart.
Citation: Câmara, E.J.N., do Prado Valladares, F.R., Santana, M.R.O. et al. High reclassification rate of height-indexed left atrial volume in obese and overweight patients with cardiac pathologies in daily clinical practice. Sci Rep 16, 6721 (2026). https://doi.org/10.1038/s41598-026-37809-z
Keywords: left atrial enlargement, obesity, echocardiography, atrial fibrillation, heart failure with preserved ejection fraction