Clear Sky Science · en
Real world outcomes of intravitreal and systemic therapy in primary and secondary vitreoretinal lymphoma
When Blurry Vision Hides a Cancer
Most people think of blood cancers as diseases of the bone marrow or lymph nodes, not the eye. Yet a rare form of lymphoma can quietly grow inside the jelly and retina of the eye, masquerading as routine inflammation and leading to months or even years of misdiagnosis. This study looks at how different eye‑directed and whole‑body treatments perform in real‑world patients with this elusive cancer, and what combinations may best keep it from coming back.
A Rare Cancer That Masquerades as Routine Eye Trouble
Vitreoretinal large B‑cell lymphoma is an uncommon but aggressive blood cancer that settles in the back of the eye. Doctors distinguish between “primary” cases that first appear in the eye and “secondary” cases in people who already have lymphoma elsewhere, such as the brain or body. Symptoms can be deceptively ordinary: blurred vision, floating spots, and a short‑lived response to steroid drops that mimic a common inflammatory disease called uveitis. Because of this disguise, diagnosis is often delayed, which matters greatly: for many patients, the disease eventually spreads to the brain and shortens survival.
How Doctors Currently Treat This Eye Lymphoma
There is no single accepted playbook for treating this cancer, so doctors often rely on local habits and individual judgment. Many patients receive tiny injections of chemotherapy directly into the eye, a method called intravitreal therapy. The two main drugs are methotrexate, an older chemotherapy agent, and rituximab, a targeted antibody drug used widely in lymphoma. Some patients receive one or the other; a few get both in sequence. Others also receive high‑dose chemotherapy through the vein, brain‑targeted treatment, or stem cell transplantation in an effort to control disease throughout the body and reduce the chance of brain involvement.
What This Two‑Center Study Set Out to Learn
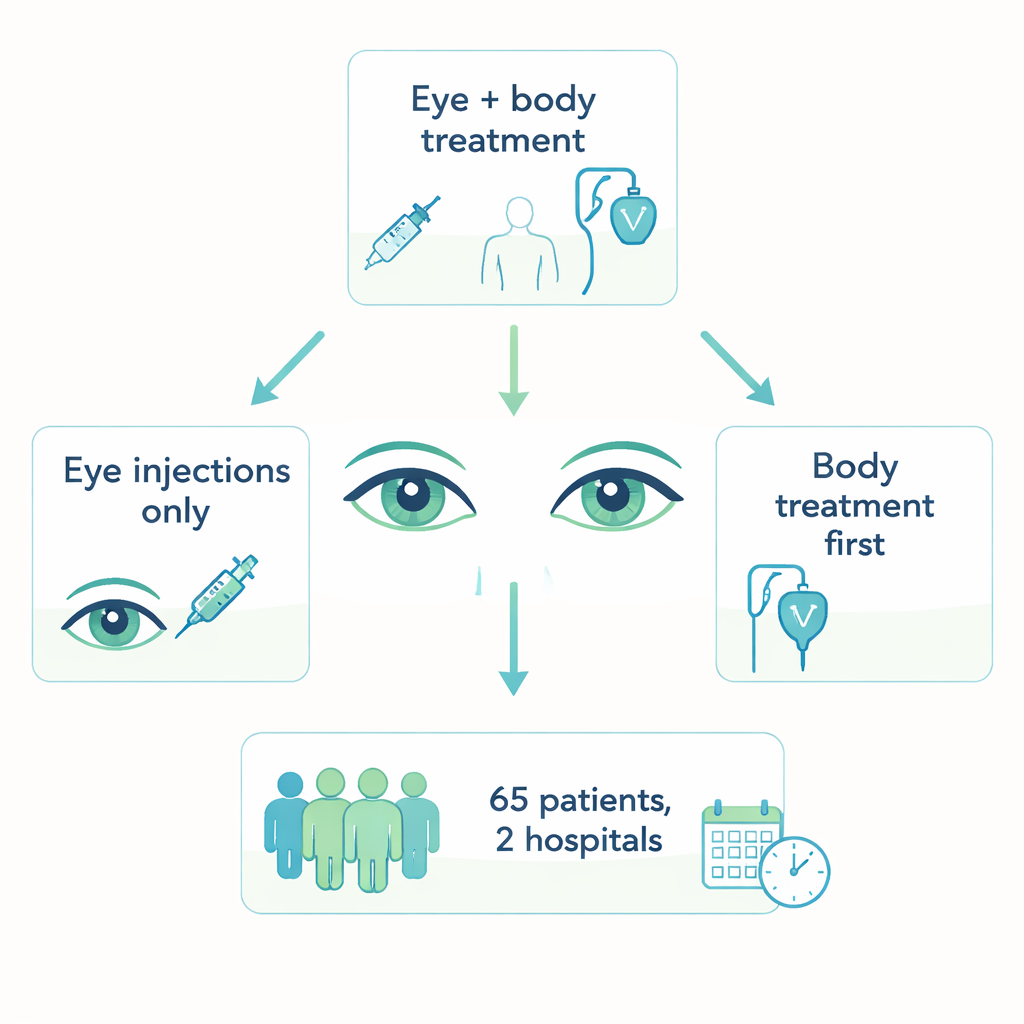
To understand which approaches work best outside of clinical trials, researchers reviewed the records of 65 patients treated at two major hospitals in Germany and Austria between 2000 and 2024. Just over half had primary eye disease, while the rest had already been treated for lymphoma elsewhere. Nearly all were older adults, with a median age in the early seventies. The team documented how long it took to reach the correct diagnosis, which treatments were used in the eye and systemically, how often the lymphoma relapsed in the eye or beyond, and what side effects occurred. A subset of 53 patients who were followed for at least nine months formed the core group for outcome analyses.
Eye Injections Alone Versus Added Whole‑Body Treatment
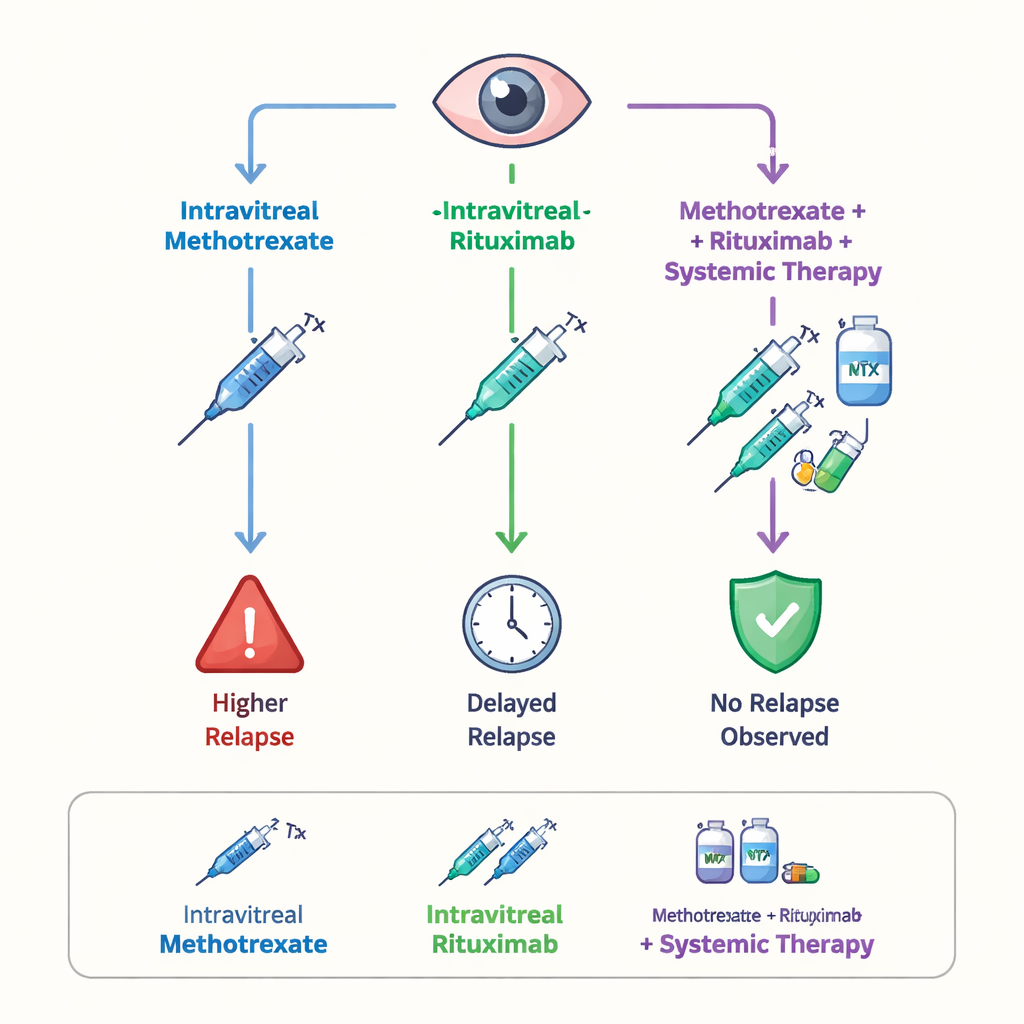
Most patients received eye injections as first‑line treatment: about half with rituximab, about a third with methotrexate, and a small group with a combination of both. Overall, relapses were common: two‑thirds of the follow‑up group had the cancer return somewhere in the body, typically within the first year. When the researchers compared the drugs, methotrexate injections showed a tendency to better protect against tumor return in the eye than rituximab alone, although the numbers were too small for firm proof. Strikingly, among the few patients who received both methotrexate and rituximab injections as part of their initial eye treatment, none experienced a relapse during the follow‑up period. Importantly, when eye injections were paired with systemic chemo‑immunotherapy, patients went longer before any relapse than those who had eye injections alone, suggesting that treating the whole body offers an added layer of protection.
Balancing Benefits and Side Effects While Preserving Sight
Each eye drug came with its own trade‑offs. Methotrexate injections frequently caused corneal surface damage, known as keratopathy, in about half of treated patients, while rituximab was more often linked to temporary spikes in eye pressure that required careful monitoring and pressure‑lowering medications. Despite these issues, overall vision sharpness remained remarkably stable from initial visit through diagnosis and after first‑line therapy, and did not differ meaningfully between the two main drugs. This suggests that, when managed carefully, intravitreal treatment can control the cancer without sacrificing sight for most patients.
What This Means for Patients and the Road Ahead
For people facing this rare eye lymphoma, the study’s message is cautiously optimistic. It indicates that direct eye injections of methotrexate, and possibly its careful combination with rituximab, may better keep the cancer at bay in the eye than rituximab alone. It also suggests that adding thoughtfully chosen systemic therapy can delay or reduce relapses beyond the eye, where the disease can be life‑threatening. However, because the cancer is so rare, the study groups were small and varied, so these results are not yet strong enough to define a universal standard of care. The work instead lays a solid foundation for future, larger trials that can rigorously test which mix of eye and body treatments gives patients the best chance of long‑lasting control with acceptable side effects.
Citation: Beer, S.A., Huber, C., Nasyrov, E. et al. Real world outcomes of intravitreal and systemic therapy in primary and secondary vitreoretinal lymphoma. Sci Rep 16, 6513 (2026). https://doi.org/10.1038/s41598-026-37804-4
Keywords: vitreoretinal lymphoma, eye cancer, intravitreal therapy, methotrexate, rituximab