Clear Sky Science · en
Agreement between Scheimpflug-based optical biometer with partial coherence interferometry in patients with keratoconus
Why this matters for people with cataracts and irregular corneas
Cataract surgery has become so precise that it often doubles as a vision-fixing procedure. But for people who also have keratoconus—an eye condition that warps the front surface of the eye—choosing the right artificial lens can be tricky. This study asks a practical question that directly affects surgical outcomes: when planning cataract surgery in keratoconus, can eye surgeons trust two common measuring machines to give interchangeable results?
Two different “rulers” for the eye
Before cataract surgery, doctors must measure the eye’s size and shape in great detail to select the best intraocular lens (IOL). This study compared two advanced optical devices used for that purpose: the IOL Master 500 and the Pentacam AXL. Both shine light into the eye and analyze the reflections, but they do so in slightly different ways and over different parts of the cornea. The researchers focused on older adults in Tehran who had both cataracts and keratoconus, looking at key measurements such as the length of the eye, the curvature of the cornea, the depth between the cornea and the natural lens, and the width of the cornea from side to side.
How the study was carried out
The team examined 121 eyes from 121 people aged over 60 years, most of them women. Everyone in the study had keratoconus and cataract but no other major eye diseases or previous eye operations. Each eye was measured with both machines in a randomized order to avoid systematic bias. Using these measurements, the researchers then calculated the recommended power of the replacement lens using six widely used formulas, including a newer one tailored specifically for keratoconus. They did not perform surgery in this project; instead, they compared how closely the two devices agreed with each other using statistical tools designed to reveal whether one machine tends to give consistently higher or lower numbers than the other.
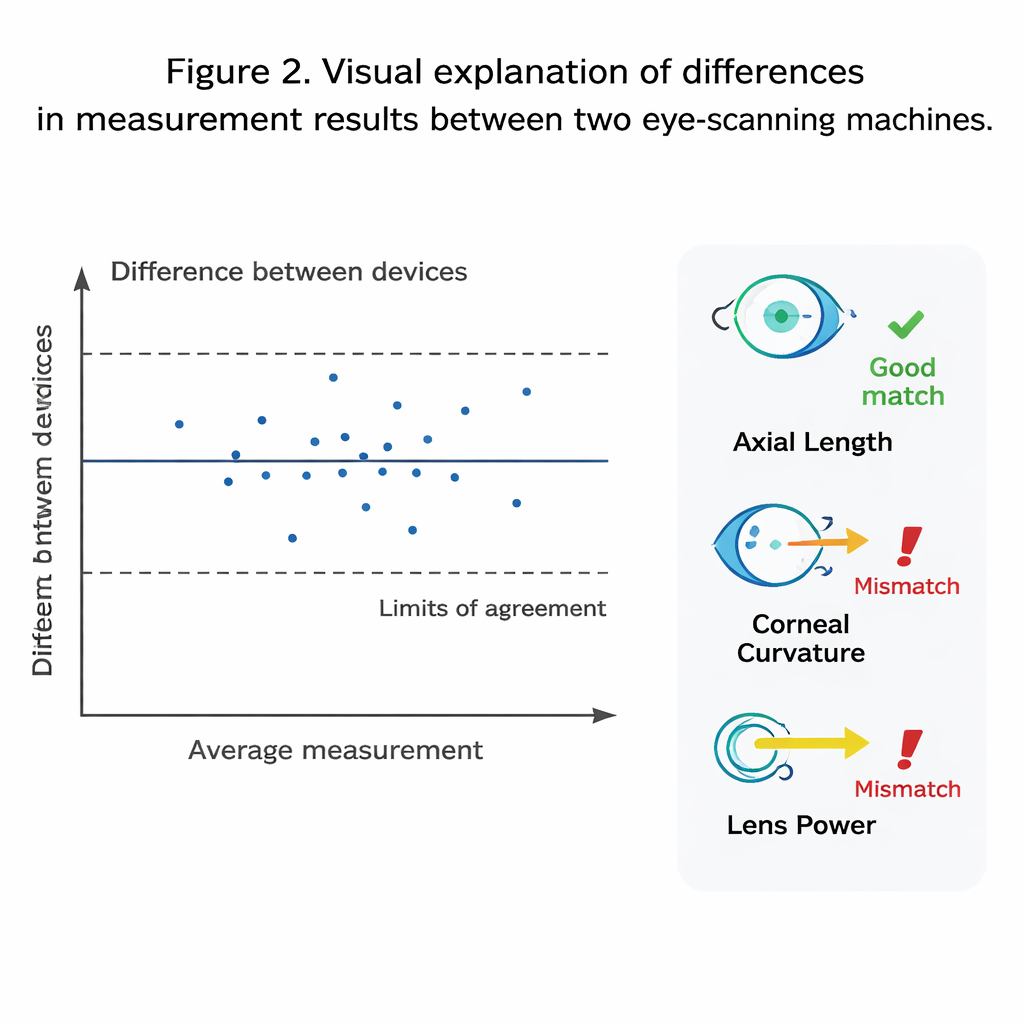
Where the machines agree—and where they don’t
The two devices were in excellent agreement when it came to the overall length of the eye. Differences were tiny—on the order of a hundredth of a millimeter—suggesting that for this particular measurement, surgeons can treat the devices as almost interchangeable. However, for other key features, such as the steepness of the cornea, the depth of the front chamber of the eye, and the white-to-white corneal width, the match was much poorer. The IOL Master 500 generally measured the cornea as steeper, the front chamber as shallower, and the eye’s width as larger than the Pentacam AXL did. These small geometric discrepancies matter because lens power formulas are very sensitive to such inputs, especially in eyes already distorted by keratoconus.
Impact on choosing the replacement lens
When the researchers fed each device’s measurements into six different IOL formulas, the Pentacam AXL consistently produced higher recommended lens powers than the IOL Master 500, by around 0.4 diopters on average and sometimes up to about 2 diopters. That size of difference can translate into noticeable under‐ or over-correction after surgery. The size of the disagreement also depended on which formula was used. Several traditional formulas showed a “proportional bias,” meaning the gap between the devices grew in eyes that required stronger lenses. In contrast, two formulas—Holladay 1 and especially the Kane keratoconus formula—showed more stable behavior across the full range of powers, although Holladay 1 still performed less reliably overall in this keratoconus group.
What this means for patients and surgeons
For people with keratoconus undergoing cataract surgery, this study delivers a clear but nuanced message: while the two devices are effectively interchangeable for measuring how long the eye is, they should not be swapped freely for the more delicate measurements that drive lens selection. Because the Pentacam AXL tends to suggest slightly stronger lenses, and because some formulas handle keratoconus better than others, the authors recommend that surgeons stick with a single device and carefully choose or adjust their formulas—favoring options like the Kane keratoconus or SRK/T formulas—rather than mixing measurements across machines. In plain terms, the measuring tool and the math formula both matter, and getting them right together can improve the chances of sharp, glasses-free vision after cataract surgery in eyes with keratoconus.
Citation: Hashemi, H., Jamali, A., Ahmad, M.A. et al. Agreement between Scheimpflug-based optical biometer with partial coherence interferometry in patients with keratoconus. Sci Rep 16, 6216 (2026). https://doi.org/10.1038/s41598-026-37513-y
Keywords: cataract surgery, keratoconus, intraocular lens power, ocular biometry, Pentacam versus IOL Master