Clear Sky Science · en
A validation study comparing Cheetah monitor cardiac output to thermodilution cardiac output in patients with severe mitral regurgitation
Why measuring the heart’s pumping power matters
For people with severe leakage of a heart valve, known as mitral regurgitation, doctors need to know exactly how much blood the heart pumps each minute. This “cardiac output” guides decisions about surgery, drug doses, and overall risk. In recent years, companies have marketed noninvasive monitors that estimate cardiac output through stickers on the chest, promising to avoid the discomfort and risk of inserting catheters into the heart. This study asked a simple but crucial question: in patients with significant mitral valve leakage, can one such device—the Cheetah monitor—really match the accuracy of the invasive gold‑standard test?
A closer look at a leaky heart valve
In a healthy heart, blood flows in a one‑way loop: from the lungs into the left upper chamber, through the mitral valve into the main pumping chamber, and then out to the body through the aorta. In mitral regurgitation, the mitral valve does not close properly, so with each beat some blood leaks backward instead of moving forward to the body. 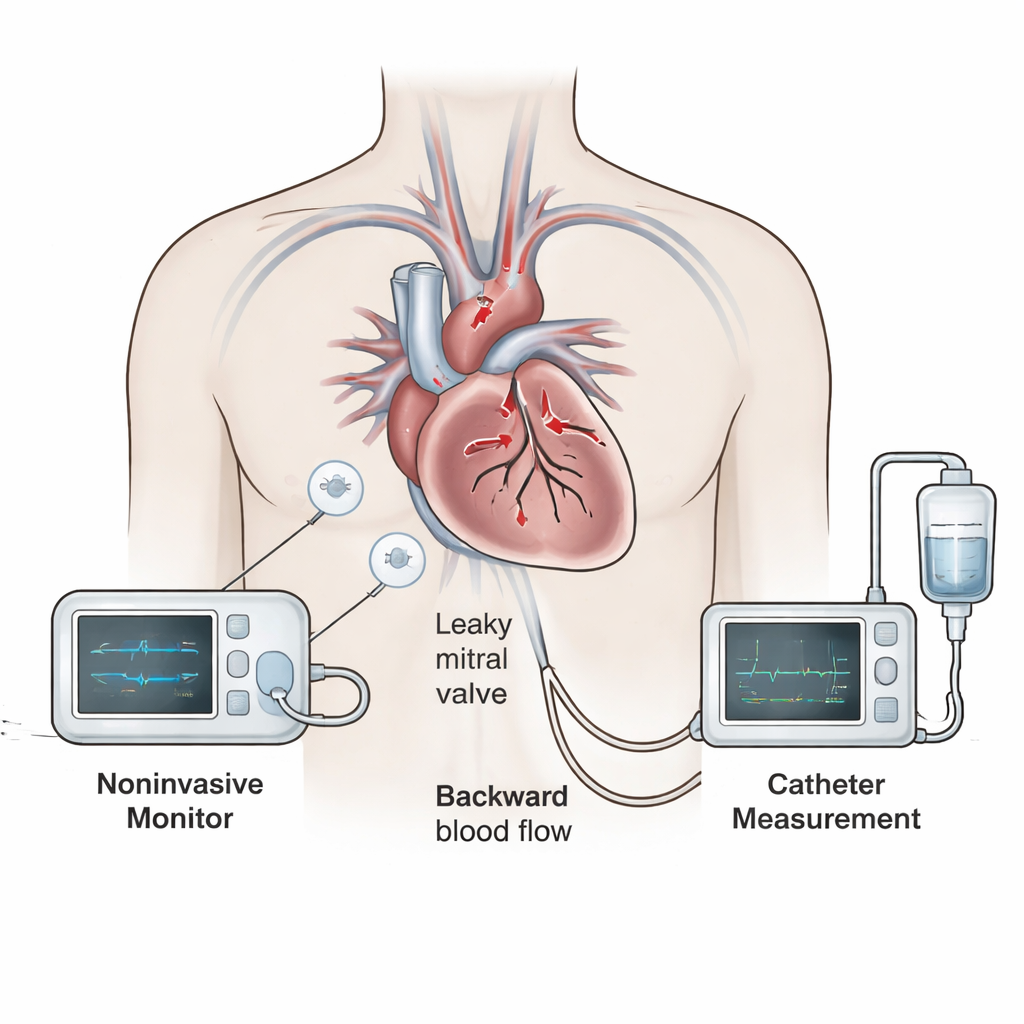
How the study was done
The researchers enrolled 26 adults with at least moderate‑to‑severe mitral regurgitation who were already scheduled for routine right and left heart catheterization before valve surgery. While these patients were sedated but breathing on their own, the team measured cardiac output in three ways: with the Cheetah monitor on the chest, with the thermodilution catheter in the heart, and with a calculation method called the modified Fick technique that uses blood oxygen levels and an estimated oxygen consumption. By comparing readings taken at the same time, they could see how closely the newer methods tracked the catheter standard and whether differences were small enough to be clinically acceptable.
What the comparisons revealed
When the researchers compared the Cheetah readings to the thermodilution measurements, they found that the two rarely agreed closely. On average, the Cheetah monitor read almost one liter of blood per minute higher than the catheter method, and in some patients the difference was several liters per minute in either direction. Almost half of all paired measurements differed by more than one liter per minute, a gap large enough to influence treatment decisions. Statistical checks also showed that this spread of differences was wide and irregular, meaning that the device might be close to correct in one patient and far off in another, even at similar true cardiac outputs. 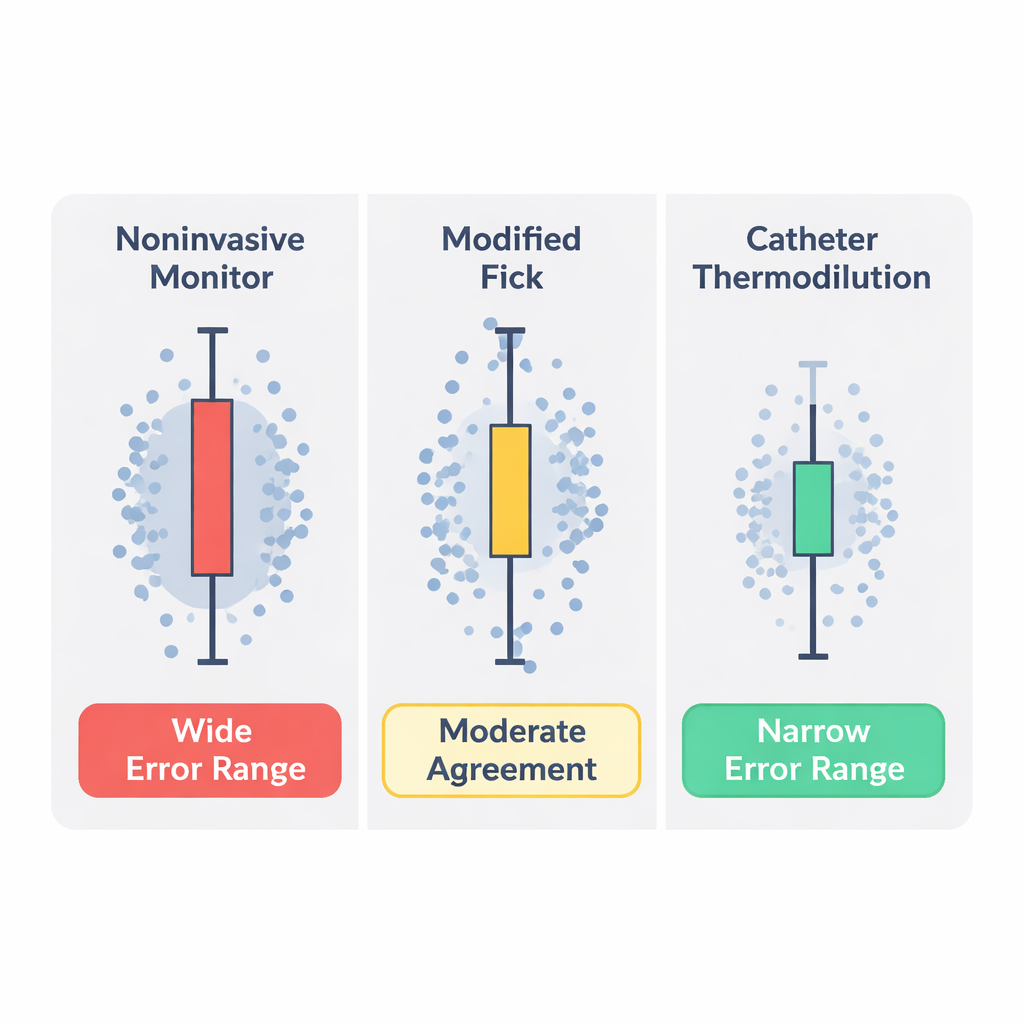
An alternative method fares a bit better
The team also compared the modified Fick calculations to the thermodilution results. Here, the average difference was small—less than a quarter of a liter per minute—and the range of disagreement, while still notable, was narrower than with the Cheetah monitor. The Fick method relies on estimating how much oxygen a person uses at rest, which is known to introduce its own errors, but in this group it showed a moderate overall match with the catheter standard. Earlier and larger studies have similarly suggested that, while not perfect, the modified Fick approach can be useful when thermodilution is not available.
What this means for patients and clinicians
For patients with significant mitral valve leakage, the study delivers a clear practical message. In this setting, the noninvasive Cheetah monitor did not provide readings that could safely replace those from the invasive thermodilution catheter. Overestimating how much blood the heart pumps by roughly a liter per minute could mislead doctors into thinking a weak heart is performing better than it really is, with consequences for timing of surgery or choice of medications. The authors stress that their findings apply to people with moderate to severe mitral regurgitation and do not rule out the monitor’s usefulness in those without valve leakage. Still, until better validated tools are available, the catheter‑based thermodilution method remains the most reliable way to measure cardiac output in these high‑risk patients, with the modified Fick method serving as a reasonable backup when invasive monitoring is not feasible.
Citation: Mitrev, L., Rosenbloom, M., Kaddissi, G. et al. A validation study comparing Cheetah monitor cardiac output to thermodilution cardiac output in patients with severe mitral regurgitation. Sci Rep 16, 6306 (2026). https://doi.org/10.1038/s41598-026-37478-y
Keywords: mitral regurgitation, cardiac output monitoring, thermodilution, noninvasive cardiac output, Cheetah monitor