Clear Sky Science · en
Modified Müller’s muscle conjunctival resection combined with levator plication in moderate to severe congenital ptosis with poor levator function
Why droopy eyelids in children matter
Some children are born with one upper eyelid that droops so far down it partly covers the pupil. This is more than a cosmetic issue: it can block vision, blur sight by changing the eye’s focusing shape, and affect a child’s confidence at school. Surgeons have several ways to lift a droopy lid, but the standard operations can leave the eye looking uneven or cause trouble closing the eyelid. This study tested a modified technique that aims to open the visual axis and give a smoother, more natural-looking eyelid in young patients with especially weak lifting muscles.
A new twist on an existing operation
The droopy lid in these children, called congenital ptosis, is usually blamed on a weak main lifting muscle in the upper eyelid. Traditionally, surgeons either connect the lid to the forehead muscle with a “sling” or shorten the main lifting muscle from the front. Both options can work but often lead to side effects such as difficulty closing the eye, dry spots on the cornea, scars on the skin, or an uneven eyelid curve. Another, less visible operation works from inside the eyelid, removing a strip of inner muscle and lining called Müller’s muscle and conjunctiva. That internal method is usually reserved for milder drooping in patients whose eyelids respond to a test eye drop. The authors wondered whether a strengthened version of this internal surgery, combined with a small tightening of the main lifting muscle, could help children with more severe droop and very weak eyelid muscles.
How the combined procedure is done
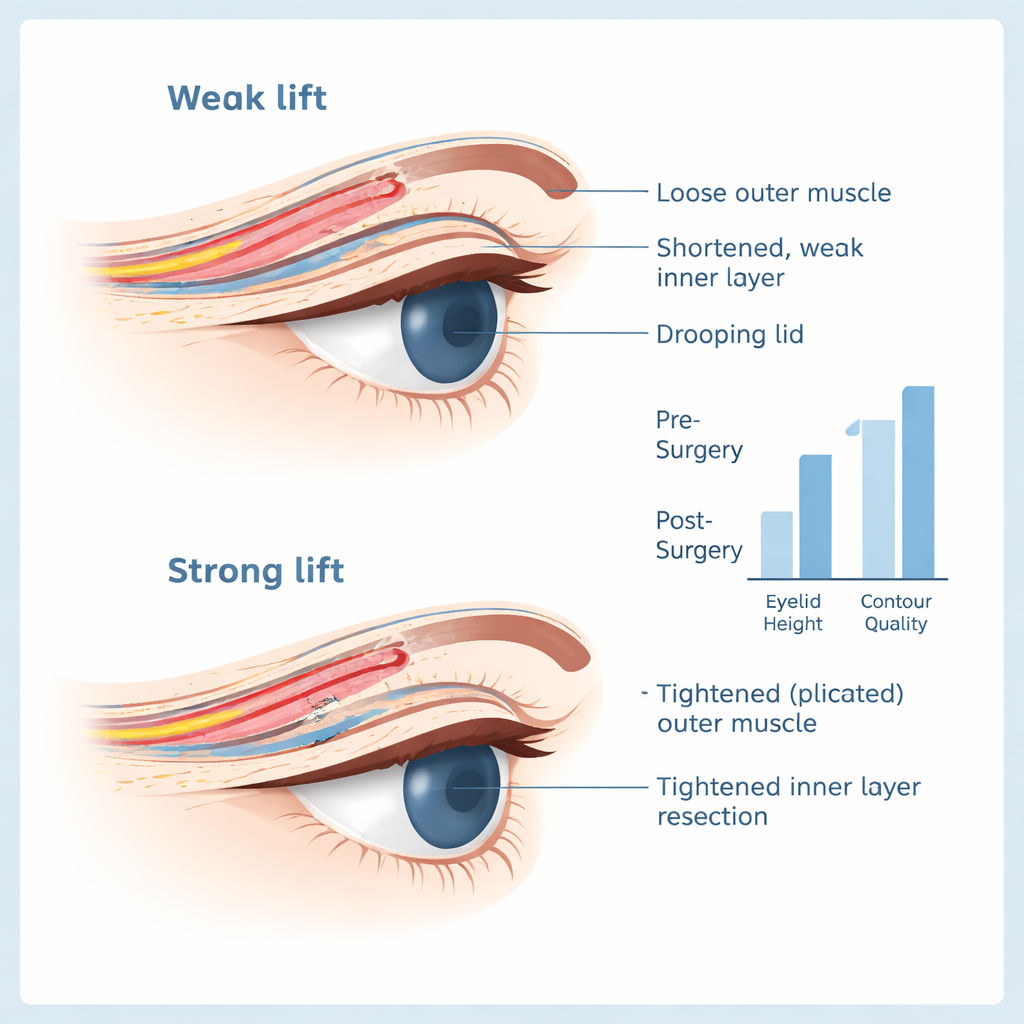
The team in Tehran enrolled 34 children and teenagers, aged 1 to 18, each with one moderately to severely droopy eyelid and poor lifting strength. Under general anesthesia, the surgeon first marked three small points along the natural lid crease and made tiny skin incisions. The eyelid was then gently flipped, and a horizontal cut was made along the inner surface just above the firm tarsal plate. The inner muscle and lining were carefully separated from the main lifting tendon up to a supporting structure high in the lid. Using special sutures, the surgeon anchored this inner layer, tightened the main lifting tendon in a controlled fold (a "plication" rather than a full cut-and-shortening), passed the sutures through the firm tarsal plate and out through the skin incisions, and then removed a relatively long strip—12 to 17 millimeters—of the inner tissue. The stitches were tied and buried so that no knots were visible on the surface. Children were then treated with antibiotic and anti-inflammatory eye drops and followed over several months.
What happened to eyelid height and shape
By six months after surgery, the droopy lids had risen on average about 3 millimeters, from slightly below the pupil to a more normal position that closely matched the opposite eye. The difference in lid height between the two eyes shrank from about 4 millimeters before surgery to less than 1 millimeter afterward. The authors defined success as a lid height within 1 millimeter of the fellow eye. By this standard, about three-quarters of patients were successful, with roughly one-quarter nearly perfect and half within a barely noticeable range. Of the 25 children whose droopy lid was blocking the line of sight before surgery, 24 ended up with an open visual axis. Just as important, the overall shape of the lid border was pleasing: independent surgeons rated the eyelid curve as “excellent” in about 74 percent and “good” in another 24 percent of cases, with no child having a clearly distorted contour.
Risks, limits, and how this compares to other methods
Problems from the surgery were uncommon and generally mild. One child had short-term difficulty fully closing the eye with minor surface irritation, which improved with lubricating treatments. Another developed a small stitch-related infection that cleared with ointment. Two young children gradually lost some of the lid lift over the year but still saw well, so they did not require another operation. Unlike sling procedures, this internal approach avoided forehead scars and reduced the risk of a “frozen” upper lid that does not move well when looking down. However, the technique does remove a larger-than-usual amount of inner eyelid tissue, and the study did not follow patients long enough to rule out very late side effects. The researchers also did not analyze which pre-surgery factors best predicted success, and all operations were done by a single experienced surgeon, which may limit how widely the results apply.
What this means for children with droopy eyelids
For children and young adults with a markedly droopy eyelid and very weak lifting muscle, this strengthened internal surgery combined with tendon tightening offers a promising alternative to traditional sling or extensive front-of-the-lid operations. In most patients, it opened the line of sight and produced a natural-looking eyelid with few short-term complications. While larger, longer studies are needed, the work suggests that surgeons can increasingly choose methods that protect both vision and appearance, giving affected children a clearer view of the world and a more balanced look in the mirror.
Citation: Aghajani, A., Rafizadeh, S.M., Rajabi, M.T. et al. Modified Müller’s muscle conjunctival resection combined with levator plication in moderate to severe congenital ptosis with poor levator function. Sci Rep 16, 6224 (2026). https://doi.org/10.1038/s41598-026-37431-z
Keywords: congenital ptosis, eyelid surgery, Müller muscle conjunctival resection, levator plication, pediatric ophthalmology