Clear Sky Science · en
Comparison of Oxford versus Japanese Histological Grading to predict renal function decline in IgA nephropathy: a Japanese prospective cohort study
Why kidney grading matters for patients
For people living with IgA nephropathy—a common kidney disease—it can be hard to know who will stay stable for decades and who may slowly lose kidney function. Doctors often rely on tiny samples of kidney tissue, taken by biopsy, to grade the damage and estimate a patient’s future. This study asked a practical question: when predicting long‑term kidney decline in Japanese patients, does a widely used international grading system work as well as Japan’s home‑grown system, and can using both together sharpen those predictions?
Two different ways to read a kidney biopsy
Worldwide, many specialists use what is called the Oxford classification to score IgA nephropathy. Under the microscope, pathologists look for several specific features in the filters of the kidney—such as crowding of cells, scarring, and shrinking of the working tissue—and give each one a separate lettered score. In Japan, another approach, the Japanese Histological Grade (JHG), is also common. Instead of scoring each feature separately, JHG groups the overall amount of old and new scarring into four grades, from mild (grade 1) to very severe (grade 4). Both systems aim to translate what is seen in a biopsy slide into a meaningful number that tells patients and doctors how worried they should be about future kidney failure. 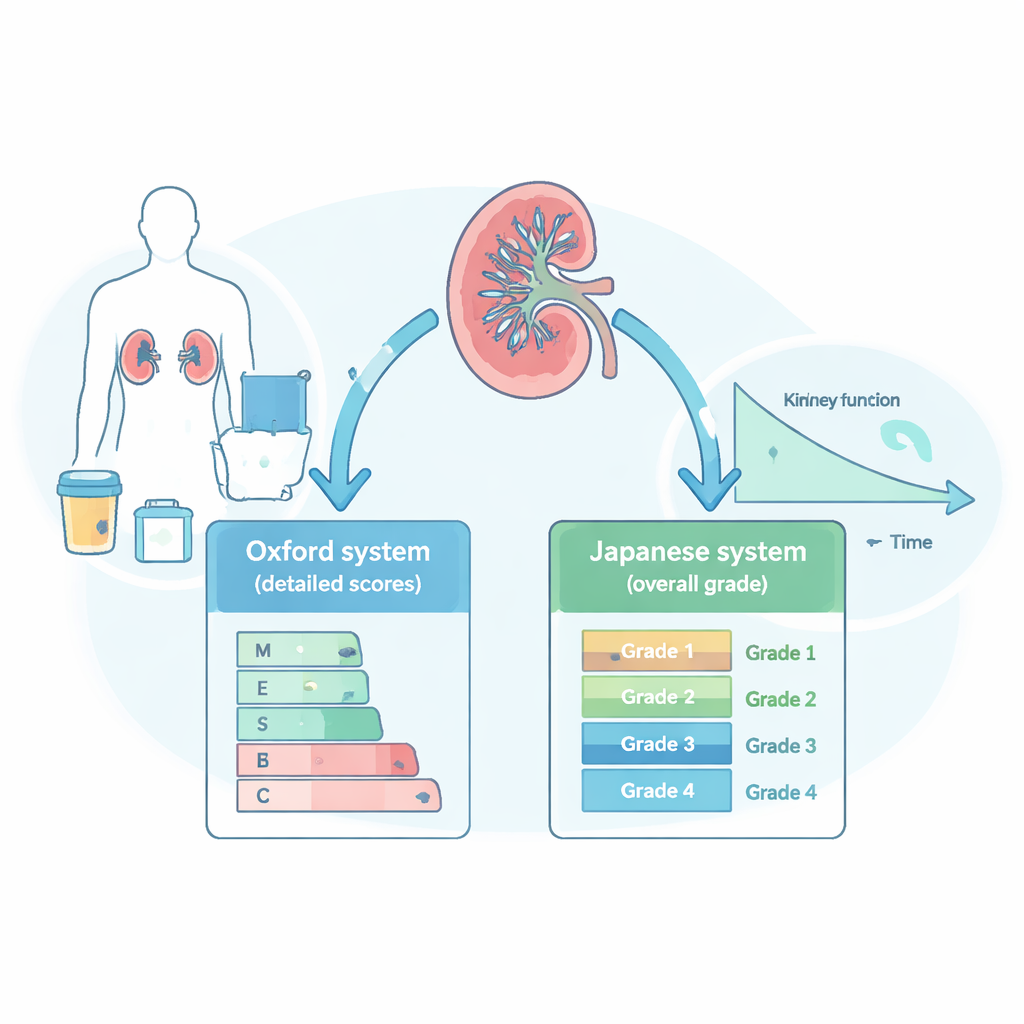
Following hundreds of patients over time
The researchers drew on a large nationwide study that had followed 938 Japanese patients with biopsy‑proven IgA nephropathy for a median of five and a half years, and in some cases up to more than 14 years. At the time of biopsy, they recorded each person’s blood pressure, kidney function (using a measure called estimated glomerular filtration rate, or eGFR), amount of protein in the urine, and whether they received common treatments such as blood‑pressure drugs that protect the kidney, steroids, or removal of the tonsils. Five expert kidney pathologists, working without knowledge of the patients’ clinical details, graded every biopsy using both the Oxford scores and the JHG system, and the team then tracked who went on to lose at least half of their kidney filtering capacity or developed kidney failure requiring dialysis.
Which grading system predicted decline better?
Both grading approaches turned out to be strong predictors of major kidney decline. When the researchers built statistical models using only the biopsy information, the Oxford scores and the Japanese grades each separated high‑risk from low‑risk patients with similar accuracy. In particular, two Oxford features—extra cells in the kidney’s filtering areas and scarring of the supporting tissue—were closely linked to later kidney failure. Likewise, higher JHG grades (indicating more widespread scarring) showed a stepwise jump in risk, with patients in grade 4 having far higher chances of decline than those in grade 1. When the team added these biopsy grades on top of simple clinical measures such as baseline eGFR, blood pressure, and urine protein, overall prediction improved further, especially when JHG was included.
Putting the pieces together improves forecasts
The study also explored how the two systems relate to each other. As the Japanese grade increased, so did the likelihood of having the worrisome Oxford features, particularly scarring. But the relationship was not perfect, suggesting that each system captures slightly different aspects of the disease. In patients with more advanced JHG grades, the detailed Oxford scores added extra prognostic information: certain microscopic changes only clearly signaled high risk once overall scarring had passed a threshold. In contrast, among those with the mildest Japanese grade, these detailed scores mattered less, because their overall risk was already low. Taken together, these findings suggest that a “split” view (Oxford) and a “lumped” view (JHG) of the same biopsy can complement one another. 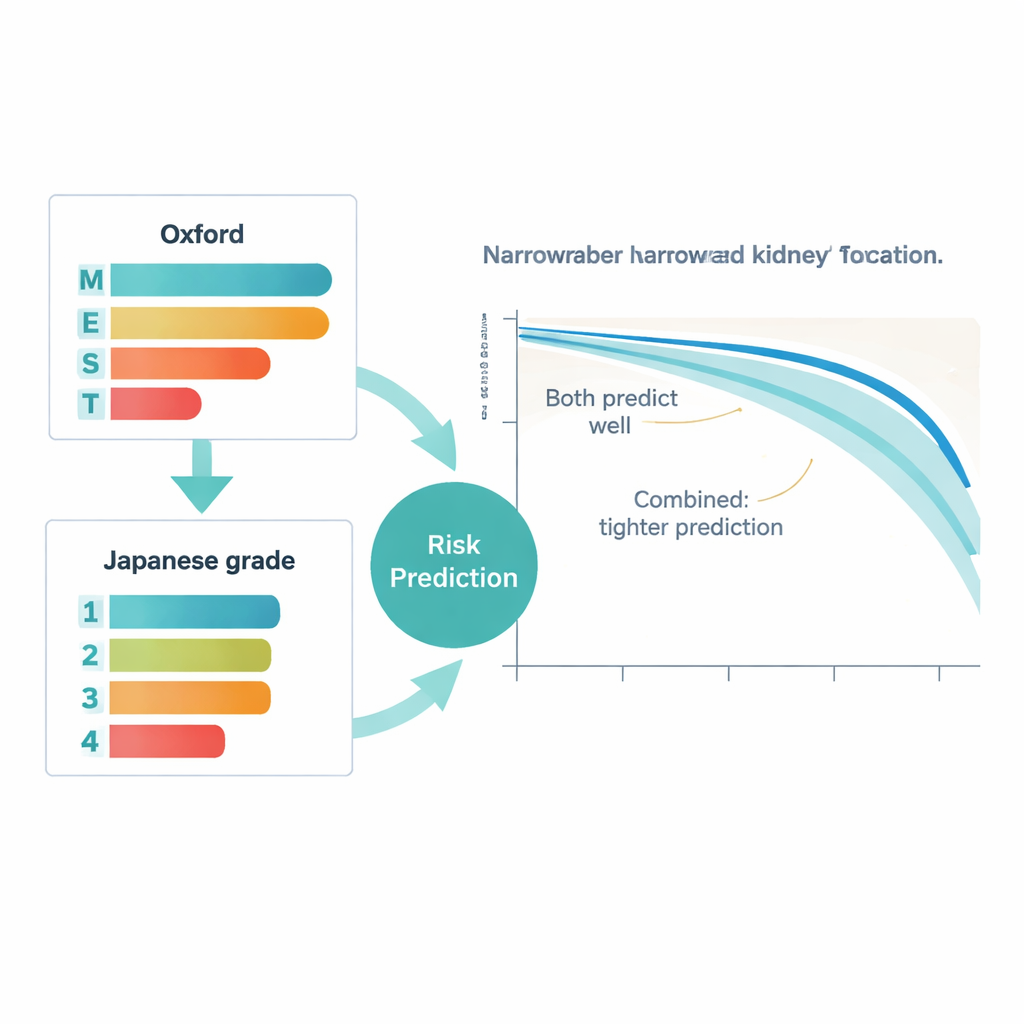
What this means for people with IgA nephropathy
For patients and clinicians, the message is reassuring and practical. Simple clinical measures like kidney function and urine protein at the time of diagnosis already provide a strong sense of long‑term outlook. Adding either of the two major biopsy grading systems improves that forecast, and using both together may give the sharpest picture of who needs closer monitoring or more aggressive treatment. While these results come from Japanese patients and need to be confirmed elsewhere, they support a future in which biopsy readings are translated into clearer, more individualized risk estimates—helping people with IgA nephropathy and their doctors make more informed decisions about care.
Citation: Sakaguchi, R., Joh, K., Honma, S. et al. Comparison of Oxford versus Japanese Histological Grading to predict renal function decline in IgA nephropathy: a Japanese prospective cohort study. Sci Rep 16, 6995 (2026). https://doi.org/10.1038/s41598-026-37412-2
Keywords: IgA nephropathy, kidney biopsy, renal function decline, histological grading, prognosis prediction