Clear Sky Science · en
Expression of CD38+CD8+ T cells in hepatitis B-related acute-on-chronic liver failure and its prognostic value
Why this liver study matters
Chronic hepatitis B is common worldwide and can silently damage the liver for years. In some people, this smoldering disease suddenly worsens into a crisis called acute-on-chronic liver failure, where jaundice, bleeding problems and multi‑organ failure can appear within days. Doctors urgently need better ways to tell which patients are heading for recovery and which are at high risk of dying. This study explores whether a particular type of immune cell in the blood can serve as an early warning signal.
A closer look at a dangerous liver crisis
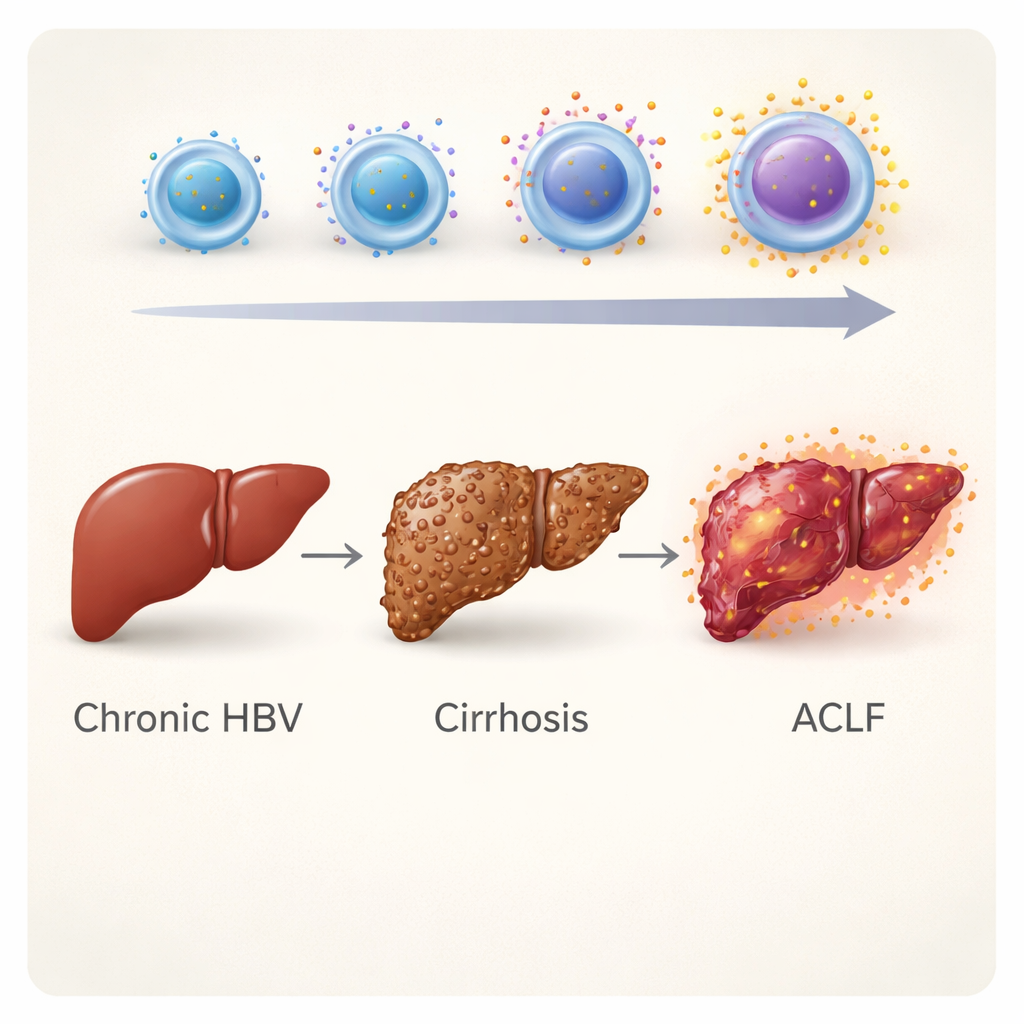
Acute-on-chronic liver failure (ACLF) happens when an already damaged liver suddenly deteriorates, often after a new trigger such as infection, stopping hepatitis B medication or heavy drinking. Patients may rapidly develop fluid in the abdomen, confusion from liver‑related brain injury and serious infections. Standard hospital scores, such as the MELD and Child–Pugh scores, estimate how sick the liver is by using lab tests like bilirubin and clotting time. However, these tools say little about how the immune system is behaving, even though immune overreaction and exhaustion are central to ACLF. The researchers set out to find an immune marker that tracks this imbalance more directly.
The immune cell clue: CD38 on killer T cells
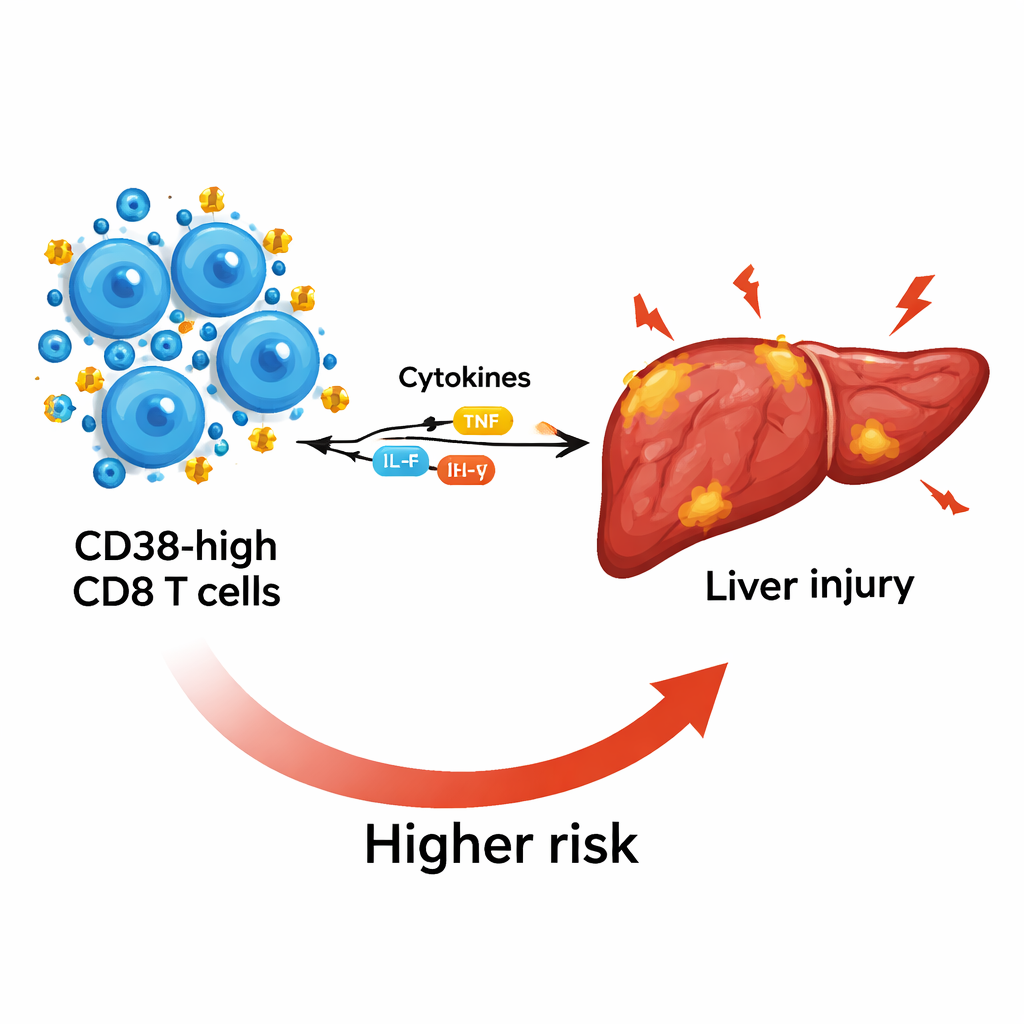
The team focused on CD8 T cells, sometimes called “killer” T cells, which normally help clear virus‑infected cells. They studied 180 people divided into three groups: chronic hepatitis B without major scarring, hepatitis B–related cirrhosis, and hepatitis B–related ACLF. Using flow cytometry, a technique that counts and characterizes cells in blood, they measured how much of a surface molecule called CD38 was present on several immune cell types. Among all the cells tested, CD8 T cells carrying high levels of CD38 stood out. These CD38‑high CD8 T cells were far more common in patients with cirrhosis and especially in those with ACLF than in people with milder chronic hepatitis B, suggesting a link to more advanced disease.
How this marker tracks inflammation and liver damage
To understand what these cells might be doing, the scientists examined inflammatory substances called cytokines in the blood. Patients with ACLF had strongly raised levels of both “pro‑inflammatory” cytokines, which drive tissue damage, and “anti‑inflammatory” cytokines, which can suppress defenses and promote infection. Higher CD38 levels on CD8 T cells went hand in hand with higher levels of key cytokines such as IL‑6 and IL‑10, indicating that these cells sit at the crossroads of harmful inflammation and immune paralysis. CD38 levels also rose in step with markers of worse liver injury, including higher bilirubin and an unfavorable AST/ALT ratio, and fell as platelet counts—a sign of the liver’s remaining reserve—dropped.
Predicting who improves and who gets worse
The researchers then followed a subset of ACLF patients over several weeks of treatment. In those who clinically improved, CD38 on CD8 T cells steadily decreased. In contrast, in patients who deteriorated, CD38 levels stayed high or even rose further. People who developed infections, a frequent and deadly complication in ACLF, also had higher CD38 levels than those who did not. When the team compared survivors and non‑survivors at three months, patients who died had clearly higher CD38 intensity on their CD8 T cells. Statistical analyses showed that this single immune measure was an independent predictor of death at both 28 days and three months.
Combining old and new tools for prognosis
Because doctors already rely heavily on the MELD score, the authors asked whether adding CD38 information could sharpen its predictive power. They found that combining CD38‑high CD8 T cell levels with the MELD score improved the ability to forecast three‑month death risk compared with MELD alone, and performed better than another common marker, the neutrophil‑to‑lymphocyte ratio. This suggests that a simple blood immune test, layered onto existing scoring systems, could help identify which hepatitis B patients with ACLF most urgently need intensive care, closer monitoring or consideration for liver transplant.
What this means for patients and care
For non‑specialists, the message is that the study has uncovered a promising “immune thermometer” for a life‑threatening liver crisis. Measuring CD38 on CD8 T cells appears to mirror how inflamed and exhausted the immune system is, how damaged the liver has become and how likely a patient is to recover. Although larger trials are needed before it becomes part of routine practice, this marker—and future treatments that might target the same pathway—could eventually help doctors personalize care and improve survival for people facing the sudden crash of hepatitis B–related liver failure.
Citation: Li, J., Li, H., Du, S. et al. Expression of CD38+CD8+ T cells in hepatitis B-related acute-on-chronic liver failure and its prognostic value. Sci Rep 16, 6609 (2026). https://doi.org/10.1038/s41598-026-37404-2
Keywords: hepatitis B, acute-on-chronic liver failure, immune biomarker, CD8 T cells, liver prognosis