Clear Sky Science · en
Refractory eosinophilic duodenal bulb ulcer associated with Helicobacter pylori eradication in children: a multicenter study
When Treating One Stomach Problem Uncovers Another
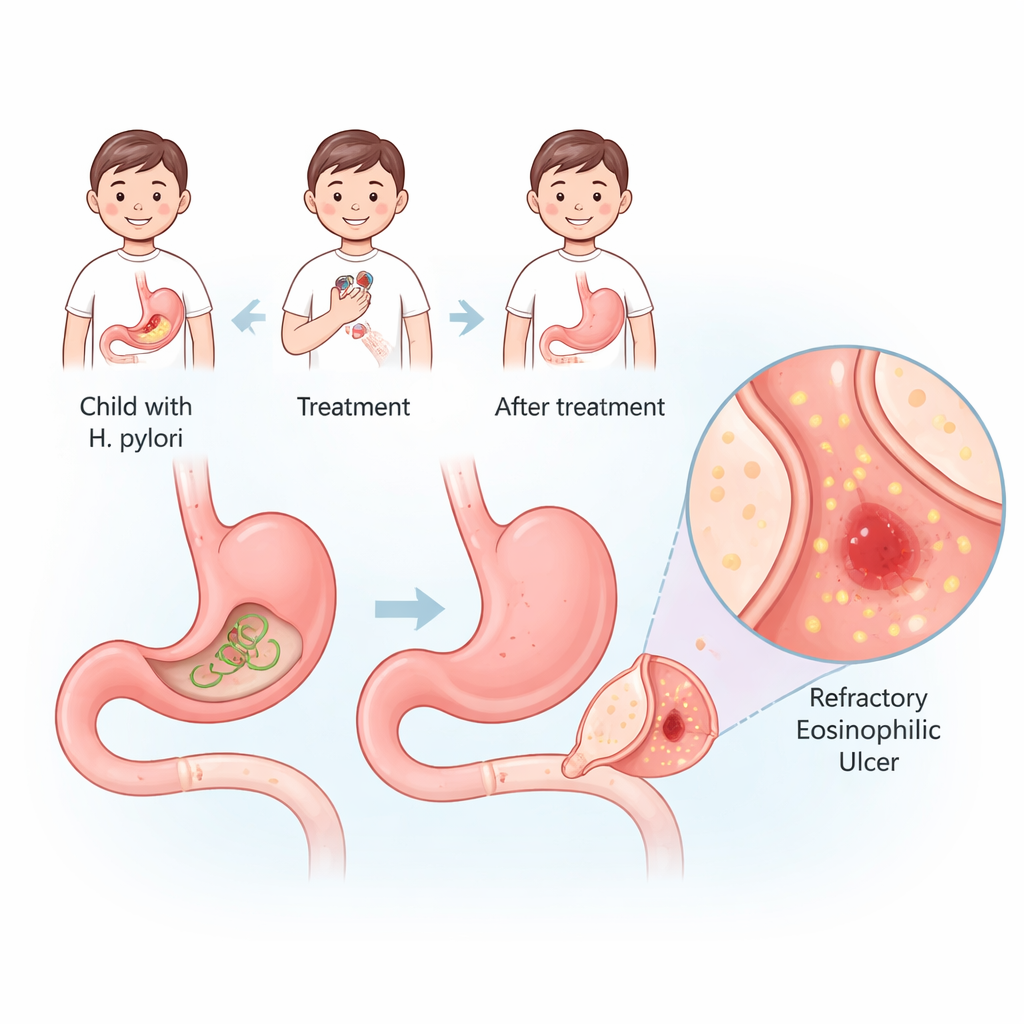
Stomach infections caused by the bacterium Helicobacter pylori are common in children and can lead to painful ulcers. Doctors usually celebrate when this microbe is wiped out with antibiotics. But this study shows that, in a small group of children, curing the infection was followed by a new and stubborn kind of ulcer in the first part of the small intestine. Understanding why this happens matters to any parent or clinician who assumes that getting rid of one problem always restores a child’s gut to perfect health.
A Rare but Troublesome Type of Ulcer in Kids
The researchers focused on children with an unusual condition called refractory eosinophilic duodenal bulb ulcers, or REDU. These ulcers sit in the duodenal bulb, where the stomach empties into the small intestine. They are “refractory” because they do not heal easily and tend to come back, and “eosinophilic” because they are packed with a type of white blood cell involved in allergies. By reviewing records from three children’s hospitals over nearly a decade, the team identified 30 children with REDU. Nineteen developed their ulcers after standard treatment to clear H. pylori, while eleven had no sign of the bacterium and were labeled idiopathic, meaning no clear cause was found.
How These Children Looked and What Doctors Found
Most affected children were school age (average around 10 years old) and boys outnumbered girls by nine to one. Abdominal pain was the main complaint, often lasting many months and driving repeated hospital visits. Many had anemia, sometimes severe enough to need blood transfusions, and more than half showed signs of poor growth or low body weight. When doctors examined the gut with an endoscope, they saw large, shallow “pan-like” ulcers in the duodenal bulb, often so big they were classified as giant ulcers. Nearly half of the children had narrowing of the duodenal bulb, which can obstruct the passage of food. Under the microscope, tissue samples from the ulcer edges were packed with eosinophils, far beyond normal levels, confirming that these were not typical acid-related ulcers.
After the Germ Is Gone, the Immune System Takes Center Stage
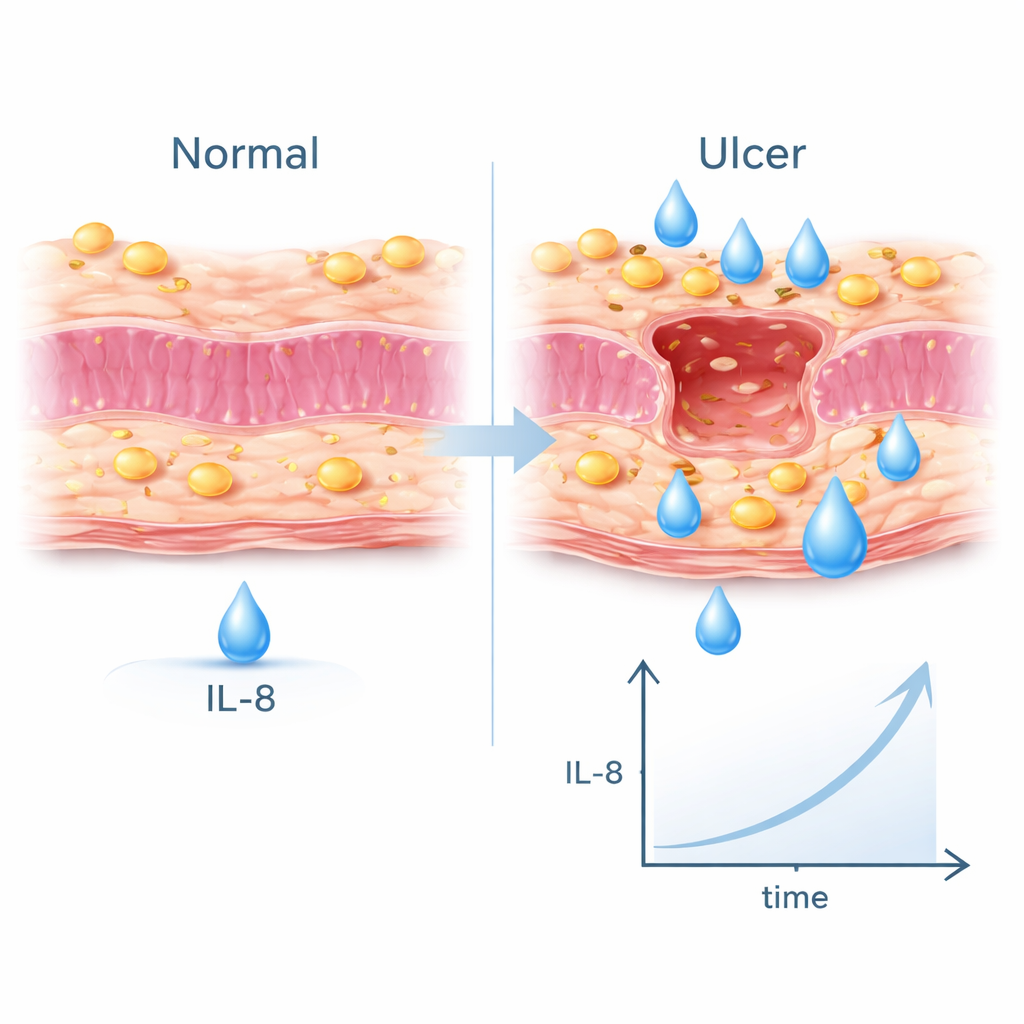
To see what made the post–H. pylori cases different, the researchers compared the 19 REDU children who had undergone eradication therapy with 38 similar children whose H. pylori-related ulcers healed normally after treatment. Children who went on to develop REDU were more likely to have giant ulcers, high eosinophil counts in the bloodstream, anemia, and repeated need for endoscopy and repeat antibiotic courses. Many also tested positive for food and environmental allergies. Blood tests for signaling molecules of the immune system revealed that one messenger, IL-8, was strikingly elevated. This points to a shift toward an allergy-like, eosinophil-heavy immune response in the gut once the original bacterium is removed.
Treatment That Helps but Rarely Cures
All children with REDU received acid-suppressing medicines called proton pump inhibitors (PPIs) and were advised to avoid trigger foods such as cow’s milk and eggs when allergies were documented. Nearly half also received steroid medicines, and about a third were given immune-suppressing drugs to keep inflammation in check. PPIs usually eased symptoms, but when doses were lowered or stopped, more than half of the children relapsed within a few weeks to months. Follow-up biopsies showed that eosinophil counts in the duodenum did fall after treatment, yet many ulcers remained stubborn. Genetic testing suggested that some children may process PPIs differently, which could partly explain why standard doses did not always work well.
What This Means for Families and Doctors
This multicenter study suggests that in a small subset of children, clearing H. pylori can upset the immune balance in the gut and open the door to a different, allergy-like ulcer disease dominated by eosinophils. For families, the key message is that ongoing belly pain, anemia, or poor growth after apparently successful ulcer treatment should not be ignored. For doctors, the findings argue for checking eosinophil levels and taking tissue samples in children with persistent duodenal ulcers, rather than assuming the infection has simply returned. While more research is needed to pinpoint the exact triggers and best therapies, this work highlights that curing an infection is not always the end of the story—and that careful follow-up can catch and manage this hidden complication.
Citation: Huang, Z., Li, P., Zhou, Y. et al. Refractory eosinophilic duodenal bulb ulcer associated with Helicobacter pylori eradication in children: a multicenter study. Sci Rep 16, 6570 (2026). https://doi.org/10.1038/s41598-026-37351-y
Keywords: Helicobacter pylori, pediatric ulcers, eosinophilic gastrointestinal disease, immune dysregulation, proton pump inhibitors