Clear Sky Science · en
The investigation of initial endotracheal tube cuff pressures in the operating room: a multi-center cross-sectional study in China
Why This Matters When You Go Under Anesthesia
Whenever someone has surgery under general anesthesia, doctors slide a breathing tube into the windpipe and inflate a tiny balloon, called a cuff, to keep air from leaking and stomach contents from entering the lungs. It sounds routine—and it is—but if that balloon is too tight or too loose, it can quietly damage the windpipe or raise the risk of pneumonia. This large study from top hospitals across China asked a simple but important question: are we actually inflating that balloon to a safe pressure in real operating rooms?
The Hidden Balloon Inside Your Windpipe
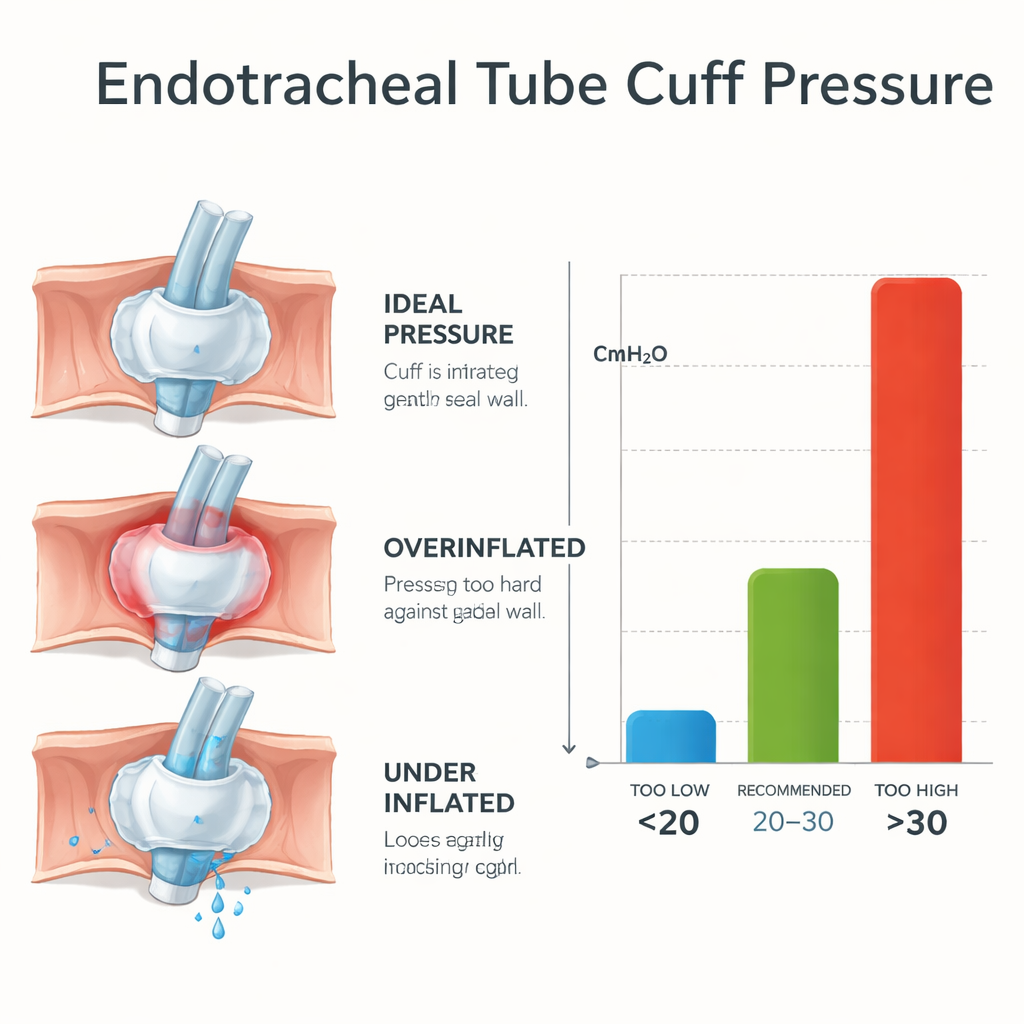
During surgery, the breathing tube’s cuff is supposed to act like a soft, gentle seal. International guidelines say its pressure should sit in a “Goldilocks zone,” not too high and not too low. Too low, and saliva or stomach fluid may slip past, potentially leading to lung infections. Too high, and the balloon can squeeze the delicate tissue of the windpipe, cutting off blood flow and causing pain, hoarseness, or even serious long‑term injury in extreme cases. Despite these risks, many anesthesia teams around the world still judge the pressure by feel, squeezing a small side balloon with their fingers instead of using a simple pressure gauge.
A Nationwide Checkup on Everyday Practice
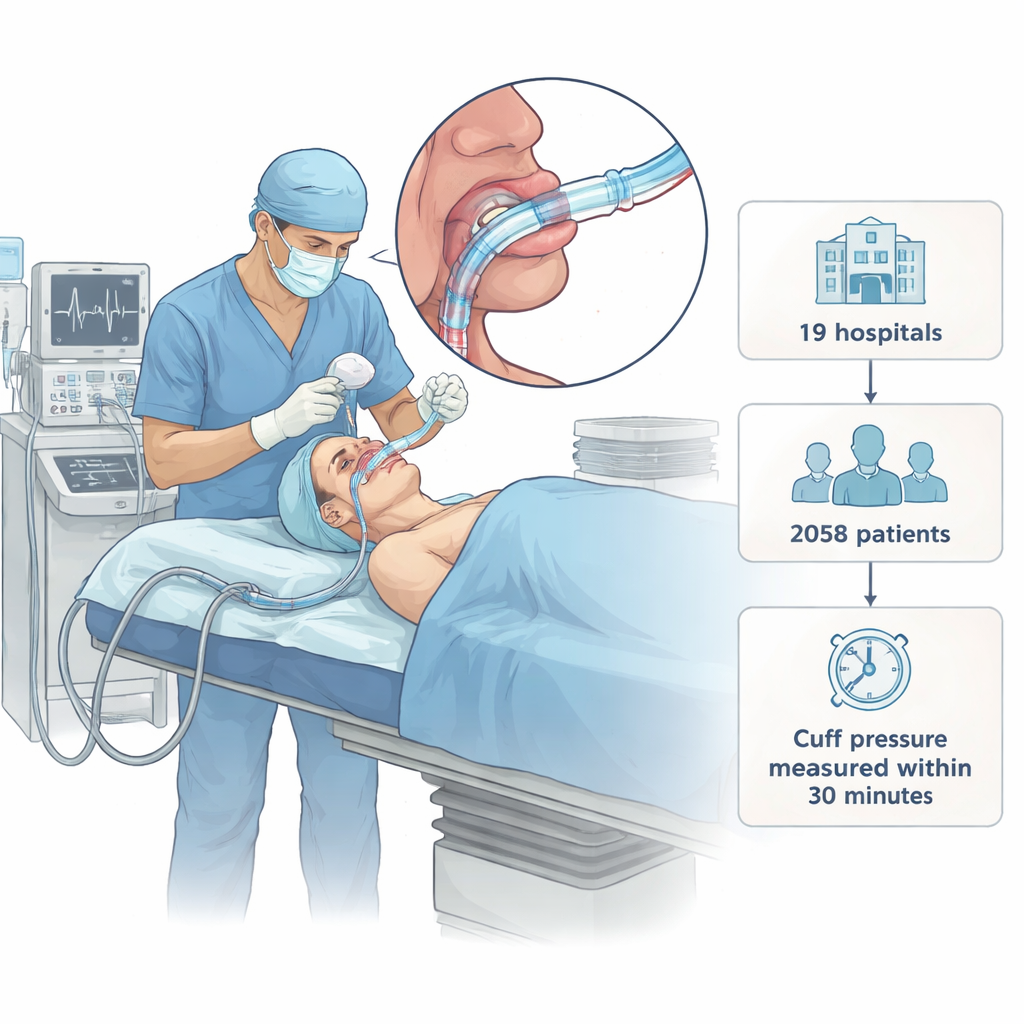
To see what really happens in busy operating rooms, researchers visited 19 top‑tier hospitals across Eastern, Central, and Western China between 2019 and 2021. They enrolled more than 2,000 adults having planned surgery with a breathing tube. Within 30 minutes after the tube was placed, a trained observer quietly attached a pressure meter to the cuff, recorded the value, and then adjusted it into the recommended range. The anesthesia teams did not see the original readings and were not told in advance how pressures would be checked, so their usual habits were left undisturbed.
What the Measurements Revealed
The results were striking. The cuff pressures ranged from very low to the upper limit of the measuring device, but the middle “safe” band was the exception, not the rule. The typical pressure was about 48 centimeters of water—well above the recommended upper limit of 30. Only about one in five patients had a pressure in the safe zone; roughly three quarters were too high, and a small minority were too low. This pattern of overinflation appeared in every hospital, even though the exact numbers varied from place to place. Almost all cuffs had been inflated using the quickest, most familiar method: squeezing the side balloon by hand. Only a handful of cases used an actual pressure gauge, and those were the only ones that reliably landed in the safe range.
Who Is Most at Risk for Too‑Tight Cuffs?
The team then looked for patterns among patients whose pressures were too high. They found that younger adults, those ventilated using a pressure‑controlled machine setting, and those breathing without a small background pressure (called PEEP) were more likely to have overinflated cuffs. Smaller‑diameter breathing tubes also tended to end up with higher pressures, perhaps because they require more air to seal the larger airway. Another important clue pointed to human factors: when cuff inflation was handled by trainees—residents, interns, or other clinicians in training—overinflation was more common than when experienced staff took charge. These patterns suggest that both equipment choices and training strongly shape how safely the cuff is managed.
What Needs to Change
Despite decades of guidance, this study shows that routine cuff management in well‑resourced hospitals still falls far short of best practice. Relying on “feel” instead of measurement makes it very hard to hit a narrow safe range, and adding more air to the cuff often seems harmless in the moment. The authors argue that using a simple pressure gauge should become standard, not optional, much like using a blood pressure cuff instead of guessing by a pulse. They also highlight the need for focused teaching and supervision so that trainees learn to treat cuff pressure as a vital safety check rather than an afterthought.
What This Means for Patients
For people facing surgery, the message is both cautionary and reassuring. The caution is that a small, invisible detail of anesthesia care is often not handled as precisely as it should be, even in leading hospitals. The reassurance is that the fix is straightforward: routine use of pressure meters and better training can sharply reduce the risk of over‑tight cuffs and the throat problems and airway injuries that can follow. In other words, by paying close attention to this tiny balloon, operating room teams can make anesthesia a little safer and recovery a little more comfortable for millions of patients.
Citation: Peng, H., Tang, Z., Li, Y. et al. The investigation of initial endotracheal tube cuff pressures in the operating room: a multi-center cross-sectional study in China. Sci Rep 16, 6856 (2026). https://doi.org/10.1038/s41598-026-37279-3
Keywords: general anesthesia, endotracheal tube, cuff pressure, patient safety, airway management