Clear Sky Science · en
Machine learning for predicting functional outcomes in acute ischemic stroke: insights from a nationwide stroke registry
Why predicting stroke recovery matters
Stroke strikes suddenly, and families often want to know: “Will my loved one walk, talk, and live independently again?” Doctors must make urgent treatment decisions with limited time and information, yet accurately predicting recovery is still difficult. This study from a nationwide Korean stroke registry shows how modern computer programs, known as machine learning models, can combine many pieces of medical data to forecast how well patients will function by the time they leave the hospital—and which treatments most strongly tilt the odds toward a better life.
A nationwide snapshot of stroke care
The researchers analyzed records from 40,586 people admitted with acute ischemic stroke—the most common type, caused by a blocked blood vessel in the brain—across roughly 220 hospitals in South Korea. The average patient was about 69 years old, and stroke severity on arrival was generally moderate. The team drew on a rich set of information: age, sex, smoking, heart rhythm problems, other illnesses, how quickly patients reached the hospital and received brain scans, which treatments they received (such as clot-busting drugs, clot-removal procedures, surgery, and rehabilitation), and what kind of hospital care unit they were admitted to. By discharge, 63.6% of patients achieved what doctors call a “good functional outcome,” meaning they were independent or only mildly disabled in daily activities.
Treatments that tip the balance
Several aspects of care stood out as strongly linked to better day-to-day functioning at discharge. Patients who received mechanical thrombectomy—a procedure in which doctors thread a catheter into a blocked brain artery to physically remove the clot—were more than twice as likely to leave the hospital with good function, even though they typically started out with more severe strokes. Rehabilitation therapy also showed a powerful benefit: patients who received targeted rehab during their stay had nearly three times the odds of a favorable outcome. Younger age and less severe stroke on arrival were associated with better recovery, while a heavier burden of other illnesses predicted worse results. Interestingly, people who smoked and those treated with timely clot-busting drugs also tended to have better outcomes, echoing a controversial “smoker’s paradox” seen in other studies, though this finding may be influenced by complex biological and care patterns.
Teaching computers to forecast recovery
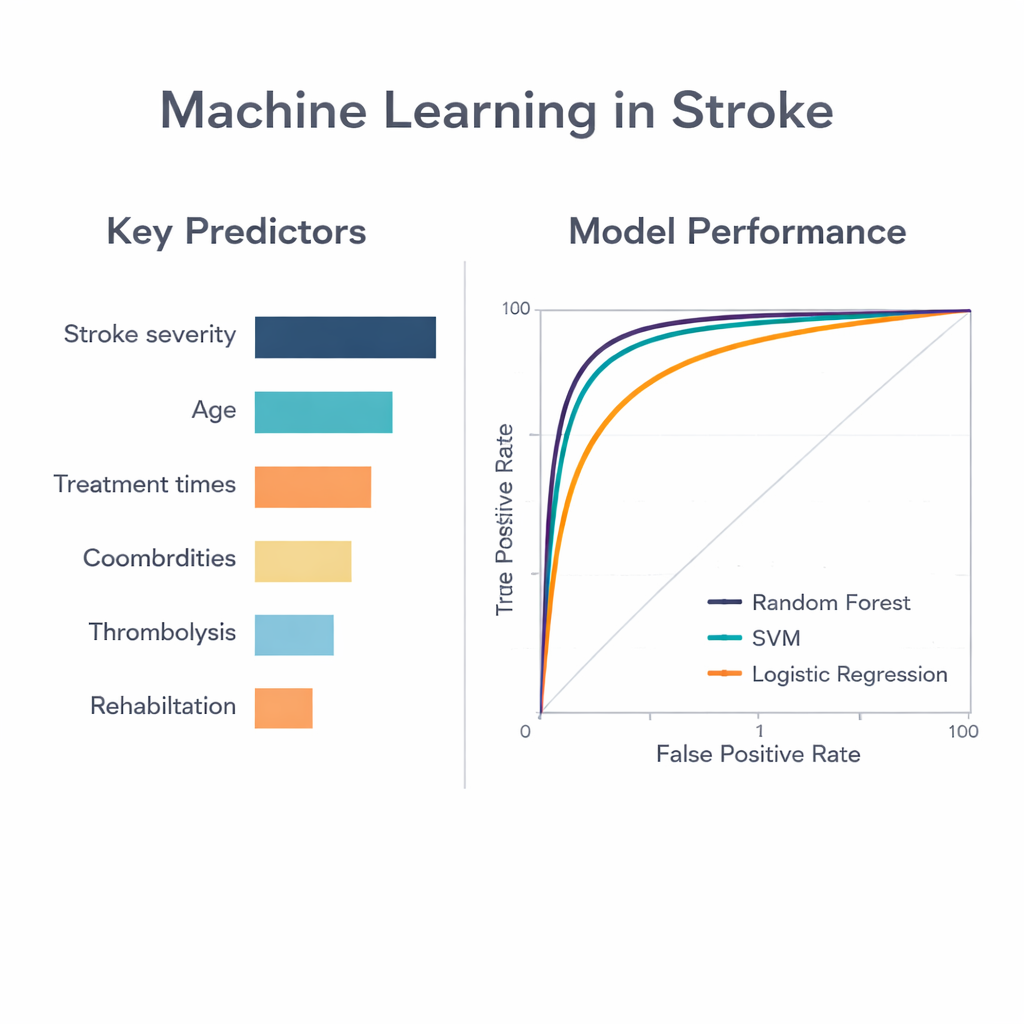
To move beyond traditional one-size-fits-all prediction scores, the team trained three types of computer models to predict who would have good function at discharge: a random forest model, a support vector machine, and standard logistic regression. All three took in the same set of routinely collected clinical and treatment variables. The random forest model—an approach that combines many decision trees and lets them vote—performed best, correctly distinguishing good from poor outcomes with an accuracy measure (area under the curve) of 0.87. The other two methods reached 0.80. This means the random forest model was better at capturing subtle, nonlinear patterns in how stroke severity, age, timing, and treatments interact to shape recovery for each individual.
What matters most to the model
By probing the inner workings of the random forest, the researchers identified which factors contributed most to its predictions. The single most important piece of information was the initial stroke severity score, followed closely by age. How quickly patients reached the hospital and received brain imaging also ranked highly, reinforcing the familiar “time is brain” message: delays can quietly erode the chances of a good outcome. Measures of overall health, use of clot-busting drugs, attention to swallowing problems, and the intensity of rehabilitation added further predictive power. Notably, some timing and swallowing-related variables appeared very influential in the machine learning model but were less clearly significant in conventional statistical analysis, suggesting that computers may be detecting complex, threshold-like effects that standard methods miss.
What this means for patients and hospitals
For patients and families, the study’s message is hopeful but grounded. Recovery after stroke still depends heavily on how severe the initial injury is and how healthy the person was beforehand, but treatment choices and hospital processes make a real difference. Machine learning models like the one developed here could eventually sit in the emergency room as quiet partners, rapidly combining many data points to give doctors clearer, personalized estimates of likely recovery and to highlight the benefits of rapid treatment and early rehabilitation. Used wisely, such tools could help guide conversations, set realistic expectations, and support policies that strengthen stroke systems of care—ultimately improving the chances that more people walk out of the hospital with their independence intact.
Citation: Ko, T., Lee, K., Kwon, Y.U. et al. Machine learning for predicting functional outcomes in acute ischemic stroke: insights from a nationwide stroke registry. Sci Rep 16, 5986 (2026). https://doi.org/10.1038/s41598-026-37159-w
Keywords: ischemic stroke, machine learning, stroke prognosis, rehabilitation, random forest model