Clear Sky Science · en
Impact of donor’s acute kidney injury on graft outcomes of deceased donor kidney transplantation
Why damaged donor kidneys matter
For people with kidney failure, a transplant can mean the difference between a life tied to a dialysis machine and a return to everyday living. But there are far fewer donated kidneys than patients who need them, especially in Asian countries where waiting times can exceed a decade. This shortage has prompted doctors to ask a difficult question: is it safe to transplant kidneys from donors whose kidneys were suddenly damaged shortly before death, a problem known as acute kidney injury (AKI)?
Kidney shortage and a tough trade-off
In Korea, as in much of Asia, the number of people developing end-stage kidney disease is rising faster than in Western countries, while deceased organ donation rates remain low. That combination creates long waiting lists and pressure to use every suitable organ. Traditionally, kidneys that looked less than perfect—because they came from older or sicker donors, or from donors with AKI—were often discarded. Yet saying no to such an organ can mean years more on dialysis for a patient, with a real risk of dying before another kidney becomes available. This study asks when using these higher-risk kidneys is a smart, life-saving compromise rather than an unsafe gamble.
A nationwide look at 8,523 transplants
The researchers examined medical records from 8,523 adults who received a kidney from a deceased donor in Korea between 2008 and 2022. They divided donors into two main groups: those with AKI and those without. AKI was further graded into three stages, from milder (stage 1) to very severe (stage 3), based on how much the donor’s blood creatinine—a waste product filtered by the kidneys—had risen. They also used a score called the Korean Kidney Donor Profile Index (K-KDPI), which combines age, health problems and lab results to give an overall risk rating for how well a donor kidney is likely to perform. Finally, they tracked whether each transplanted kidney eventually failed, meaning the recipient had to resume dialysis or undergo another transplant.
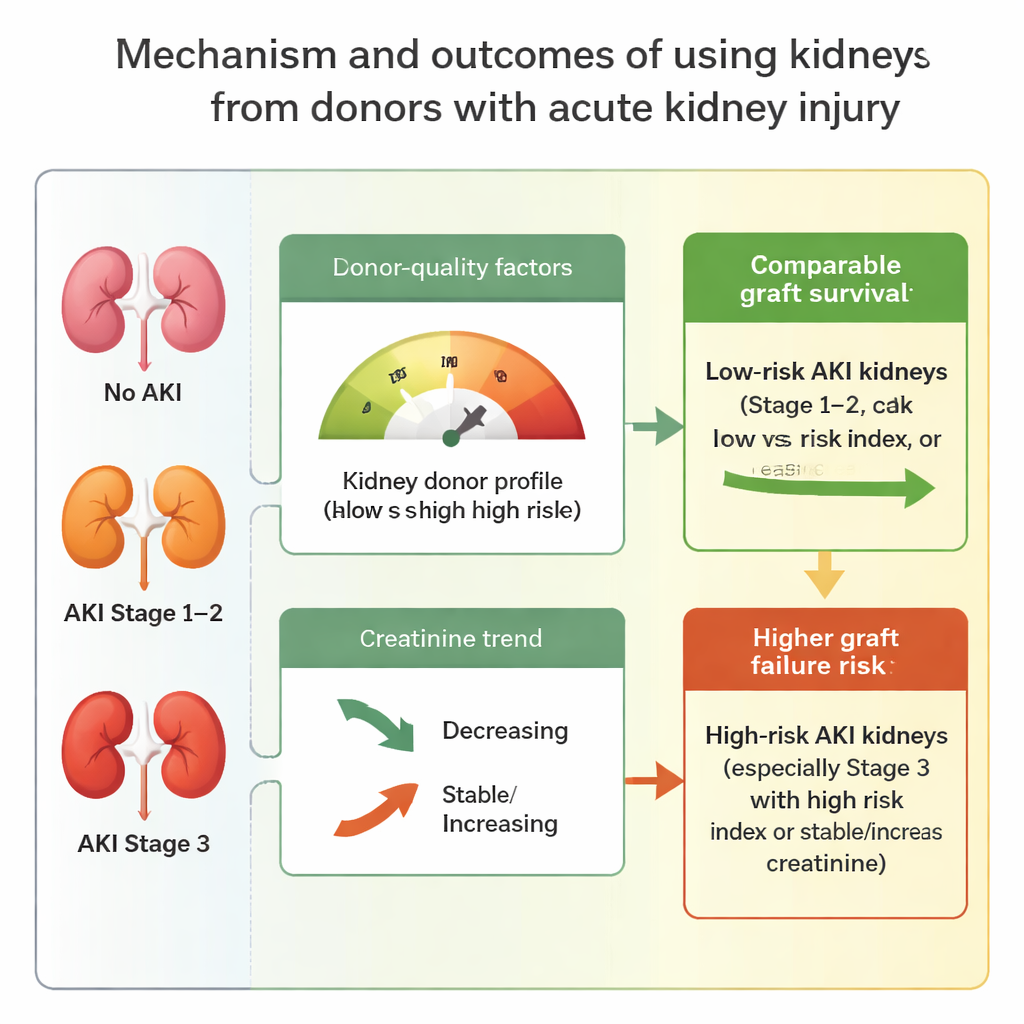
When damaged kidneys perform well—and when they don’t
Overall, recipients of kidneys from donors with AKI had a modestly higher risk of graft failure than those whose donors had normal kidney function. The increase was driven mainly by the most severe cases: kidneys from stage 3 AKI donors were more likely to fail over time. But the picture changed when the researchers looked more closely at donor quality. If the donor kidney had a relatively favorable K-KDPI score (below 70, indicating lower predicted risk), outcomes were similar whether or not the donor had AKI, even for severe AKI. Likewise, if the donor’s creatinine levels were falling before the kidney was removed—signs that the injured kidneys were starting to recover—transplanted kidneys did about as well as those from donors without AKI. In contrast, when donors had both AKI and a high-risk K-KDPI (70 or above), or when creatinine was stable or still rising, the chance of graft failure clearly increased, especially for stage 3 AKI.
Guidelines for using higher-risk organs
By combining AKI severity, donor-quality scores and creatinine trends, the study suggests practical rules for organ acceptance in settings with severe shortages. Kidneys from donors with mild to moderate AKI (stages 1 and 2) appear safe to use in most circumstances, particularly when the overall donor risk score is low or the kidney shows signs of recovery. Even some severely injured kidneys (stage 3) may be reasonable choices when the donor otherwise looks favorable. On the other hand, kidneys from donors with both severe AKI and poor overall profiles, or with no sign of creatinine improvement, carry a meaningfully higher risk and should be used more cautiously.
What this means for patients and policy
For patients facing years on dialysis in countries with long transplant waiting lists, this study offers a hopeful but nuanced message. Using kidneys from donors with temporary, recovering kidney damage can safely expand the donor pool and help more people receive life-changing transplants. The key is not to reject all AKI kidneys outright, nor to accept them blindly, but to weigh how sick the kidney was, whether it was starting to heal, and how strong the donor looked overall. With careful selection based on these factors, transplant programs—especially in Asia—can make better use of scarce organs without sacrificing long-term outcomes.
Citation: Na, O., Lee, G., Koo, T.Y. et al. Impact of donor’s acute kidney injury on graft outcomes of deceased donor kidney transplantation. Sci Rep 16, 6071 (2026). https://doi.org/10.1038/s41598-026-37147-0
Keywords: kidney transplantation, organ shortage, acute kidney injury, donor organ quality, graft survival