Clear Sky Science · en
Objective assessment of cesarean section suturing techniques using a uterine simulator
Why the Way We Stitch a Cesarean Matters
For many families, cesarean birth is a lifesaving procedure—but what happens to the uterus afterward can affect a woman’s health for years. Poorly healed cesarean scars are linked to pain, fertility problems, and risky future pregnancies. This study asked a practical question with far‑reaching consequences: can smarter suturing techniques and materials help protect women’s uteruses, even when the surgeon is still learning?
Practicing on a Safe, Artificial Uterus
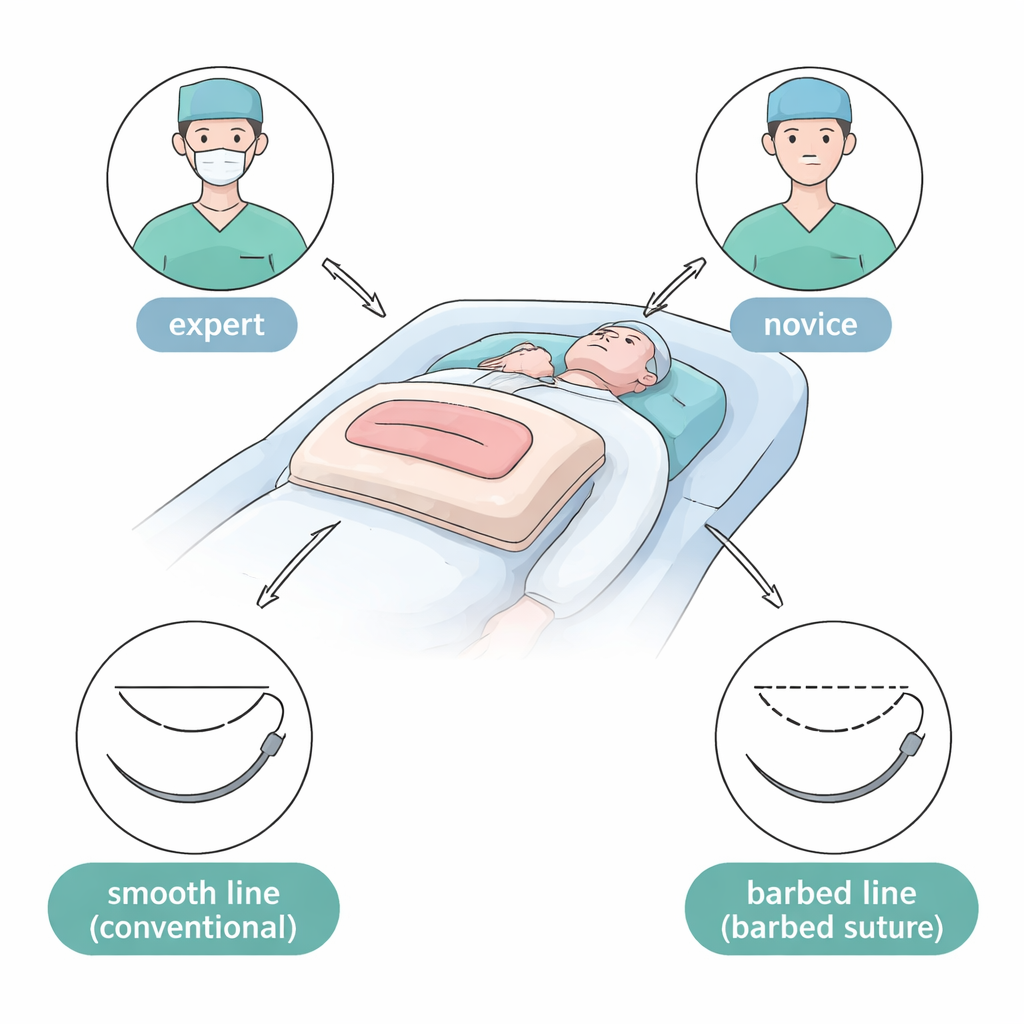
Because researchers cannot easily experiment on real patients, the team built a uterus simulator: a soft, uniform pad with a slit mimicking a cesarean incision. Obstetricians of two experience levels—30 seasoned experts and 40 junior doctors—were asked to close these artificial uteruses. They used two suture materials (traditional smooth thread and newer barbed thread that grips tissue without knots) and two common ways of stitching the uterine wall. This created eight combinations of experience, material, and technique, allowing the researchers to tease apart how each factor changed the final wound.
Two Ways to Close the Same Cut
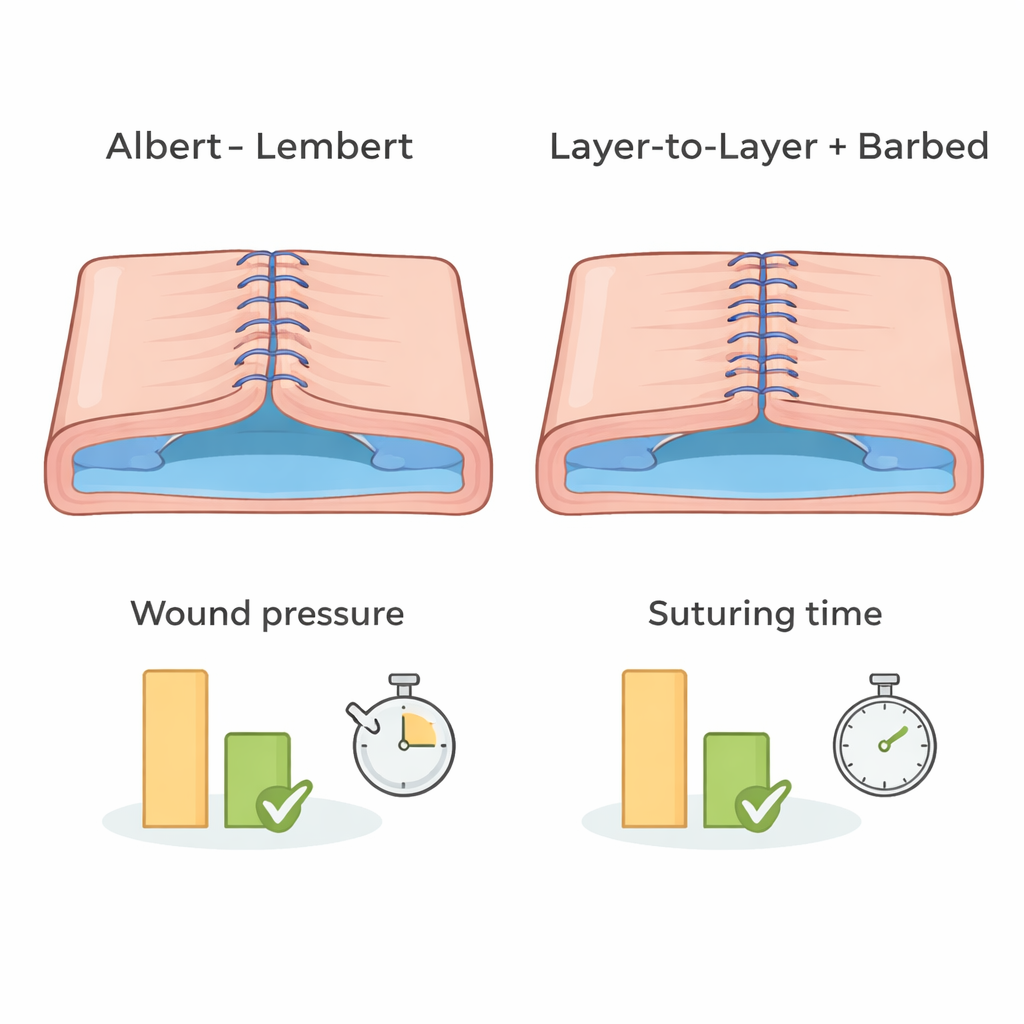
The study compared an older method, the Albert–Lembert technique, with a more straightforward “layer‑to‑layer” closure. Both involved two continuous layers of stitches. In Albert–Lembert, the first row closes the full thickness of the cut, and the second row pulls the muscle layer together to reduce tension. In layer‑to‑layer, the first row brings most of the muscle edges together and the second row simply covers and reinforces that seam, leaving part of the outer muscle untouched. Barbed sutures, unlike conventional thread, do not require knot‑tying: tiny barbs anchor each segment of the stitch, which may simplify the task for less experienced surgeons.
Measuring the “Ideal” Surgical Result
Rather than relying on visual judgment alone, the researchers defined an “ideal” wound based on how tightly and evenly it was closed without being deformed. They timed each procedure, counted stitches in both layers, and used a pressure device to test how well the closed incision resisted air leaks, a stand‑in for how securely it might hold against bleeding or internal pressure. They also measured how much the model changed shape and how large the remaining internal opening of the uterine cavity was—features that may relate to scar formation. The benchmark for “ideal” was the performance of expert surgeons using barbed sutures with the layer‑to‑layer method, a combination supported by earlier clinical studies.
How Novices Stacked Up Against Experts
When experts used barbed sutures with the Albert–Lembert method, they produced very dense stitch lines but also more distortion of the model and larger internal openings than the ideal. Novices using the same combination had similar problems. By contrast, novices using barbed sutures with the layer‑to‑layer technique needed fewer stitches and trended toward better pressure readings, coming closer to the ideal pattern than experts who used conventional sutures with the same method. In some comparisons, novices with barbed sutures matched the performance of experts using traditional thread, suggesting that the right tools and approach can partially offset limited experience—at least in a simulator.
What This Could Mean for Real Patients
The authors caution that plastic models cannot reproduce a real uterus’s blood flow, healing, or contractions, so these results do not yet prove that barbed, layer‑to‑layer closures prevent scars in living patients. Still, the simulator offered a rare, quantitative look at how experience, material, and technique interact. It showed that some combinations—especially barbed sutures with layer‑to‑layer closure—can produce more even, secure wounds with less distortion, even in the hands of beginners. For patients, the message is hopeful: as surgical training increasingly uses realistic simulators and as suture technology improves, cesarean births may become not only safer in the moment but also kinder to the uterus in the long term.
Citation: Nakato, H., Maki, J., Kuriyama, C. et al. Objective assessment of cesarean section suturing techniques using a uterine simulator. Sci Rep 16, 7456 (2026). https://doi.org/10.1038/s41598-026-37041-9
Keywords: cesarean section, uterine scar, suturing technique, surgical simulation, barbed suture