Clear Sky Science · en
Prospective randomized trial of triple port laparoscopic cholecystectomy combined with choledochoscopic common bile duct exploration and primary closure for acute abdominal pain
Why gallstones and quick recovery matter
Many people develop gallstones without ever knowing it, but when these tiny pebbles block the main bile duct, they can trigger sudden, severe abdominal pain, infection, and even life‑threatening complications. Doctors have long searched for ways to clear these stones and remove the gallbladder while causing as little trauma as possible. This study tested a streamlined keyhole surgery that uses fewer incisions and skips an external drainage tube, asking a simple but important question: can patients with serious gallstone attacks go home sooner and hurt less without sacrificing safety?

Two ways to solve the same urgent problem
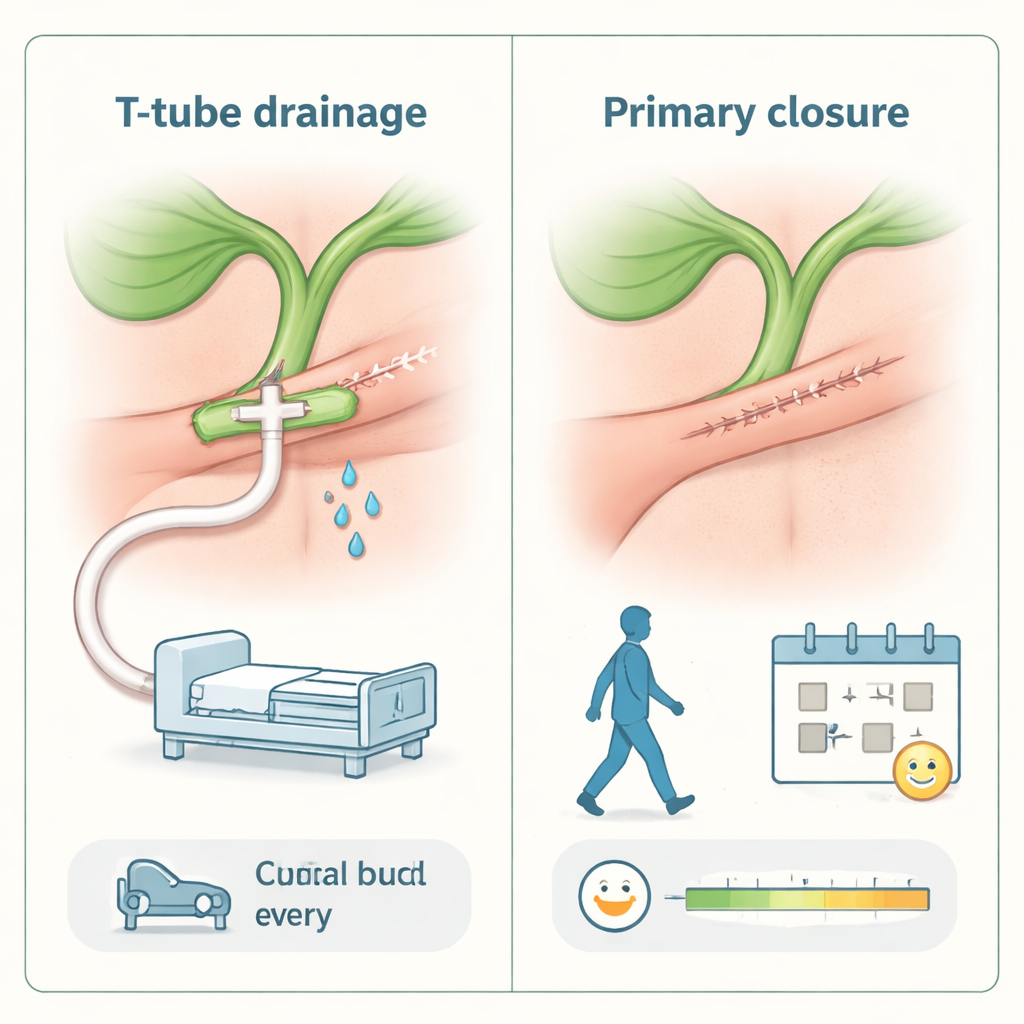
The researchers focused on patients who arrived with acute abdominal pain caused by stones in both the gallbladder and the common bile duct, often along with inflamed gallbladders. Traditionally, surgeons tackle this through minimally invasive surgery that removes the gallbladder, opens the main bile duct, clears the stones, and then leaves a rubber “T‑tube” inside the duct to drain bile to the outside for weeks. The alternative, newer approach still uses small incisions and a tiny camera, but it relies on careful inspection of the duct with a slim scope and then closes the duct directly, avoiding any external tube. This method also rearranges the working ports so the operation can be done through three small entry points instead of four.
How the trial was set up
At a hospital in Beijing, 61 adults with sudden gallstone‑related abdominal pain were randomly assigned to one of two groups. One group of 35 patients had triple‑port laparoscopic surgery with stone removal through a scope and direct stitching of the bile duct, with no T‑tube left behind. The other 26 patients underwent a similar operation but through four ports, and a T‑shaped drainage tube was placed in the duct and brought out through the skin. Both groups were comparable in age, body size, lab tests, and illness severity, and the same surgical team operated on all of them. The investigators then measured operating time, blood loss, pain on the first day after surgery, how long drains stayed in, days in the hospital, and any complications such as leaks, infections, or remaining stones.
What the surgeons and patients experienced
The triple‑port, tube‑free method came out ahead on nearly every measure of recovery. Operations were shorter by almost half an hour on average, in part because the team did not have to position and sew in a T‑tube. Blood loss was low in both groups, but slightly lower in the tube‑free group. Patients without a T‑tube reported less pain at the surgical site on the first day, had their abdominal drains removed sooner, and left the hospital earlier—shaving roughly two‑thirds of a day off their stay. Importantly, both approaches proved similarly safe in the short term: each group had just one minor bile leak that stopped on its own within a few days, and there were no deaths, no need to switch to open surgery, and no signs of leftover stones or narrowed ducts on follow‑up scans three months later.
Why a missing tube can speed healing
The study highlights several reasons why doing away with the T‑tube can help patients bounce back faster. Fewer incisions and instruments mean less trauma to the abdominal wall. Closing the bile duct directly with fine absorbable stitches avoids leaving a foreign object that can tug, leak, or require weeks of careful care and a second visit for removal. The technique also preserves the natural valve that controls bile flow into the intestine, which may reduce future trouble with stones compared with some endoscopic methods that cut this valve. By carefully choosing patients—especially making sure their bile ducts were not too narrow—and by following a strict, gentle technique for opening and closing the duct, the surgeons were able to keep complications low while aligning the operation with modern “fast‑track” recovery principles.
What this means for patients with gallstone attacks
For people struck by sudden, severe pain from gallstones blocking the main bile duct, this research suggests that a carefully performed, three‑port keyhole operation that clears the stones and closes the duct without a T‑tube can be just as safe as the more traditional method, while offering less pain and a quicker return home. The study was done at a single hospital with a modest number of patients and only three months of follow‑up, so larger, longer studies are still needed. But for surgeons experienced with this technique, the findings support moving toward simpler, tube‑free surgery that respects the body’s natural plumbing and helps patients recover more comfortably and efficiently.
Citation: Wang, X., Kang, J., Li, Y. et al. Prospective randomized trial of triple port laparoscopic cholecystectomy combined with choledochoscopic common bile duct exploration and primary closure for acute abdominal pain. Sci Rep 16, 5993 (2026). https://doi.org/10.1038/s41598-026-37034-8
Keywords: gallstones, laparoscopic surgery, bile duct stones, enhanced recovery, T-tube-free technique