Clear Sky Science · en
Weight optimization of MIMO-UWB distributed beamforming for implant communications
Smarter Wireless Links for Tiny Medical Implants
Imagine a vitamin-sized camera capsule traveling through your intestines and sending live video to your doctor. To work safely and reliably, such implants must send huge amounts of data through layers of tissue, fat, and fluid that strongly weaken radio waves. This paper explores a new way to coordinate multiple tiny devices inside the body so that, together, they can beam their signals more efficiently to an external receiver, boosting image quality and reliability without overtaxing any single implant.
Why Signals Inside the Body Are Hard to Send
Wireless body-area networks already connect sensors worn on the skin, but implants deep inside the body face harsher conditions. Traditional medical implant bands around 400 MHz are good at penetrating tissue but can only support modest data rates, enough for basic monitoring but not for real-time video. Ultra-wideband (UWB) signals in the 3.4–4.8 GHz range can carry much more information, yet these higher frequencies are strongly absorbed by body fluids and tissues. As a result, signals from a capsule endoscope can fade or drop out before reaching a wearable receiver. Simply turning up the power is not an option, because implants must be safe, tiny, and energy-frugal. Engineers therefore look for smarter ways to shape and combine radio waves so that more of the energy arrives where it is needed. 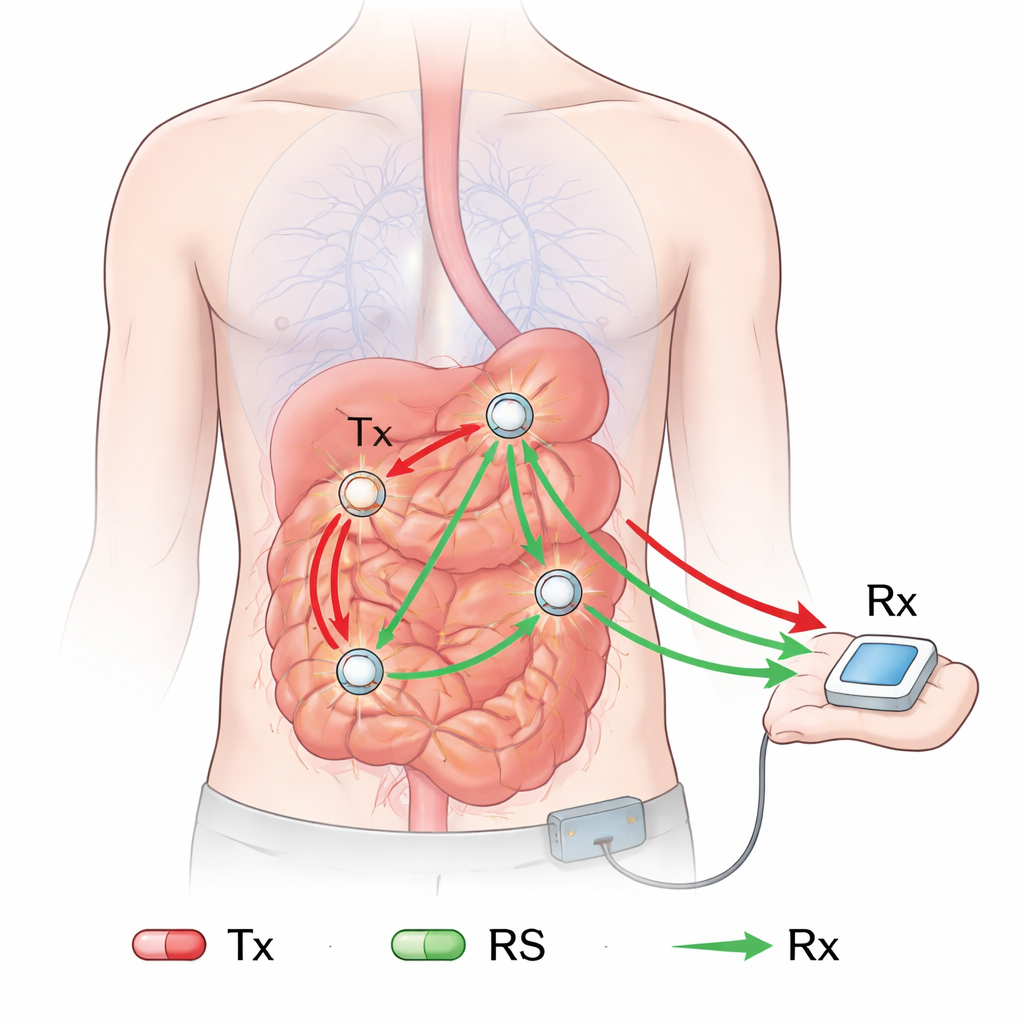
Many Tiny Devices Acting Like One Big Antenna
One powerful idea in modern wireless systems is multiple-input multiple-output (MIMO), where several antennas transmit and receive in a coordinated way to improve link quality. But squeezing several spaced antennas into a single capsule is nearly impossible. The authors instead propose treating multiple implants as a single distributed MIMO system. In their concept, a “main” capsule sends signals that are picked up by other implants acting as relay stations. These relays amplify and re-transmit the signal toward an external receiver on the body surface. Each capsule only needs one small antenna, keeping its hardware simple, while the group as a whole behaves like a multi-antenna array.
Teaching the Network to Aim Its Energy
The key innovation is a frequency-dependent distributed beamforming method tailored to the ultra-wideband channel inside the human body. Beamforming means adjusting the strength and timing (phase) of signals from different transmitters so that the waves add up constructively at the receiver. Here, the authors derive mathematical rules—weight coefficients—that tell each relay how to scale and shift its signal across the entire UWB band to maximize the effective energy per bit at the receiver. Unlike many earlier beamforming schemes, their method explicitly includes the direct path from the main capsule to the external receiver, not just the relay paths. All the heavy computations are done by the outside receiver, which has fewer size and power constraints; it then sends the needed weights back to the implants, keeping the implants themselves simple and energy-efficient.
Modeling Radio Waves Through the Human Body
To test whether this approach works in realistic conditions, the team first built a detailed model of how radio waves travel through a human torso. Using a high-resolution digital human body and a numerical technique called finite-difference time-domain analysis, they simulated UWB propagation from points inside the small intestine to multiple locations on the body surface. From these simulations, they extracted path-loss and fading parameters that describe how strongly signals are weakened and scattered. They then validated these parameters with physical experiments, transmitting UWB signals through a liquid phantom that mimics human tissue, and found close agreement between measurement and simulation.
Performance Gains for Capsule Endoscopy
With the in-body channel characterized, the authors ran extensive computer simulations for capsule endoscopy scenarios in both two-dimensional and three-dimensional layouts. They compared three cases: direct transmission without beamforming, a conventional distributed beamforming scheme that ignores the direct path, and their proposed method that optimally blends direct and relayed signals. The results show that distributed beamforming can substantially improve signal quality overall, but conventional designs can actually perform poorly when relay capsules happen to be poorly placed. In contrast, the proposed method remains robust to relay placement and consistently raises the signal-to-noise metric Eb/N0. In a realistic 3D capsule endoscopy model with moving capsules, the new scheme achieved about a 5 dB improvement over the conventional method—equivalent to making the link noticeably more reliable or allowing lower transmit power for the same performance. 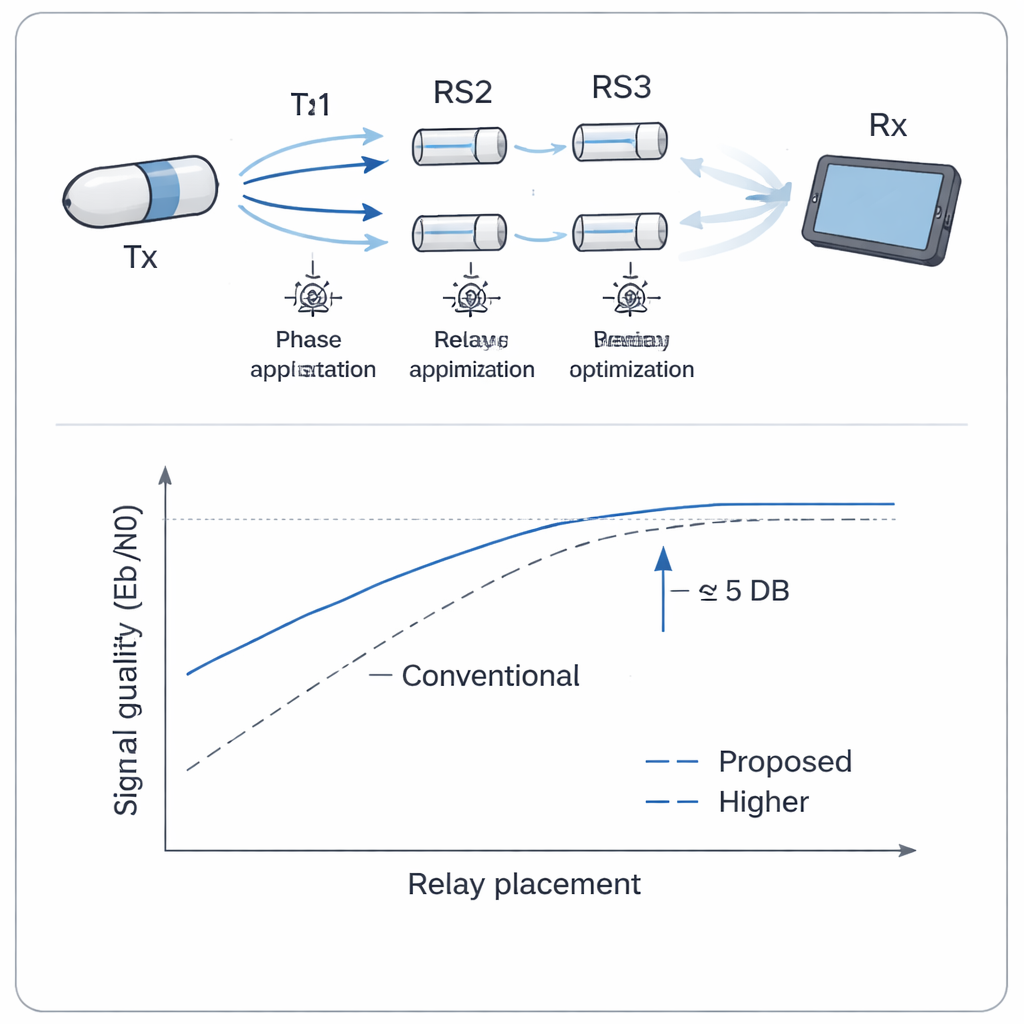
Toward Safer, More Capable Implants
In plain terms, this work shows how “teamwork” among simple implants can make wireless links inside the body both stronger and more efficient. By coordinating how multiple capsules forward and shape the same signal, and by letting an external receiver handle the complex calculations, doctors could one day obtain smoother live video and richer data from tiny ingestible or implanted devices without increasing their size or battery drain. The next steps will be to build prototype hardware, verify safety issues such as heating and specific absorption rate in animal studies, and ultimately move toward clinical systems that exploit distributed beamforming to improve the performance and safety of advanced implantable medical devices.
Citation: Kobayashi, T., Hyry, J., Fujimoto, M. et al. Weight optimization of MIMO-UWB distributed beamforming for implant communications. Sci Rep 16, 5920 (2026). https://doi.org/10.1038/s41598-026-36694-w
Keywords: capsule endoscopy, implantable medical devices, ultra-wideband communication, distributed beamforming, body area networks