Clear Sky Science · en
Evaluation of disinfection methods and effects for handwashing sinks contaminated with Pseudomonas aeruginosa
Why hospital sinks can be hidden trouble spots
In hospitals, we usually think of doctors’ hands, surgical tools, or air vents as sources of infection. Far less obvious is the humble handwashing sink. This study focuses on a stubborn germ, Pseudomonas aeruginosa, that can colonize pediatric intensive care unit (PICU) sinks and quietly spread to vulnerable children. The researchers set out to test which common disinfectants and cleaning routines actually clear this germ from sink plumbing and keep it from quickly growing back.
Germs that thrive in water and pipes
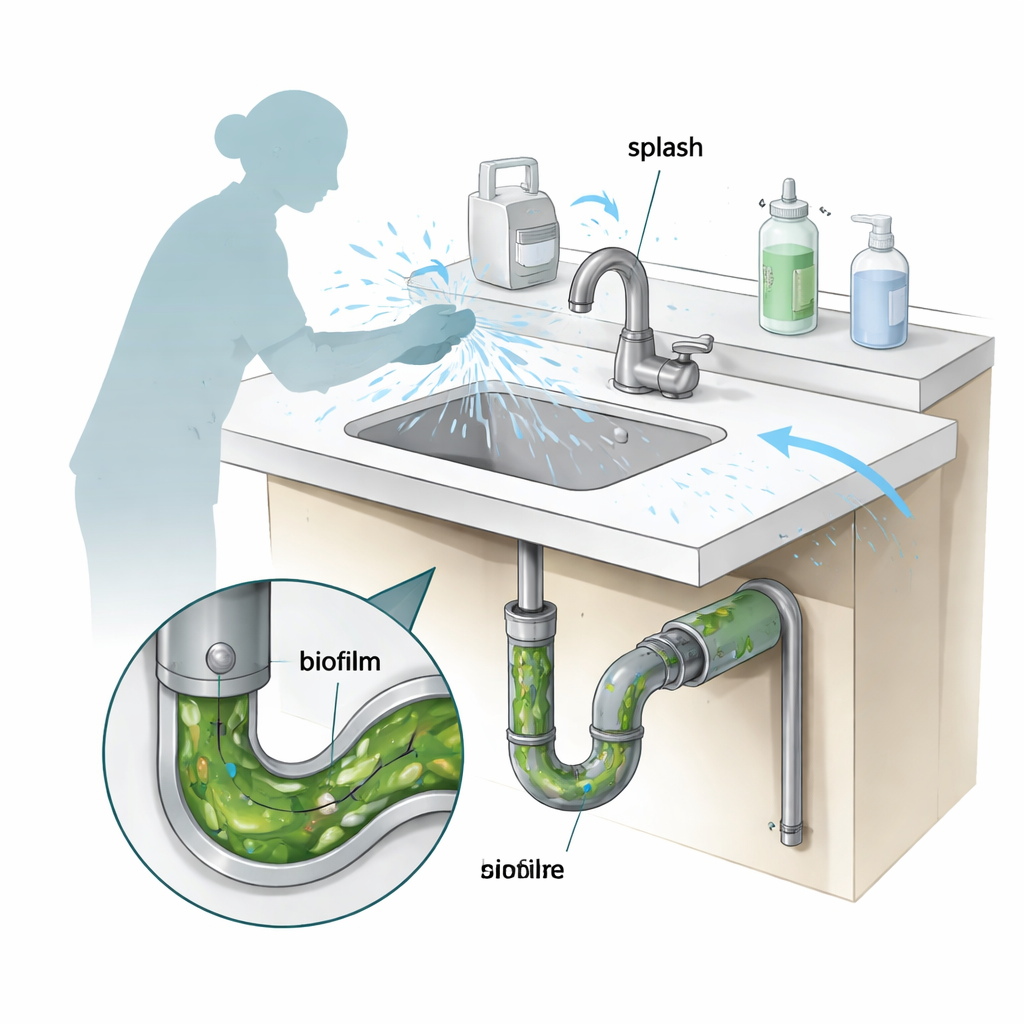
Pseudomonas aeruginosa is a hardy bacterium that loves moist, low-nutrient environments such as drains, traps, and overflow outlets. It can form slimy layers called biofilms on inner surfaces of pipes and sink hardware. Within these layers, bacteria are shielded from many disinfectants and can survive for long periods. In intensive care units, splashes from contaminated drains and contact with sink surfaces can transfer these germs to healthcare workers’ hands or nearby equipment, raising the risk of serious infections, especially in fragile newborns and critically ill children.
Testing everyday cleaning chemicals
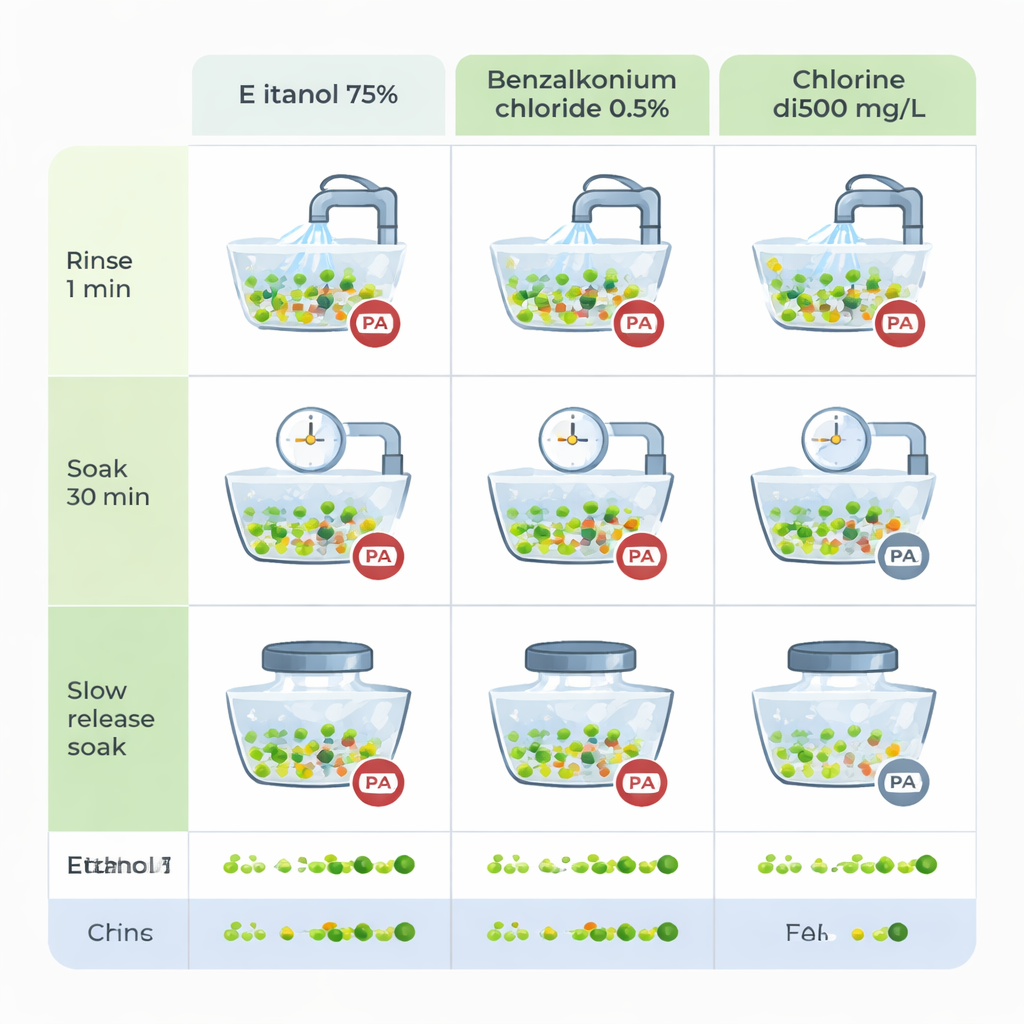
To understand which cleaning strategies work best, the team studied nine handwashing sinks in a hospital PICU that repeatedly tested positive for P. aeruginosa. Each sink was used frequently and had not recently been rebuilt or specially treated. The sinks were divided into three groups, and the researchers compared three widely used disinfectants: a chlorine-based solution (similar to diluted bleach), 0.5% benzalkonium chloride (a common quaternary ammonium disinfectant), and 75% ethanol (alcohol). For each chemical, they applied three methods: a quick rinse (flushing with disinfectant for one minute), a soaking method (filling and covering the sink and drain with disinfectant for 30 minutes), and a slow-release soaking method (slowly filling the trap beneath the sink, soaking for 30 minutes, then flushing).
Immediate knockdown versus lasting protection
The team sampled key spots—overflow outlets, drains, faucet interiors, and nearby countertop edges—before cleaning, one minute after, and 24 hours later. Ethanol gave the most dramatic instant result: within a minute, bacteria levels dropped to almost zero, and no P. aeruginosa was detected. However, this effect did not last. Because alcohol evaporates quickly and does not penetrate deeply into biofilms, the germ reappeared within a day. Chlorine-based disinfectant also killed large numbers of bacteria, and unlike ethanol, it provided the best 24‑hour suppression of P. aeruginosa. Benzalkonium chloride performed worst: even after treatment, substantial bacterial residue often remained, and the target germ was still detected in about a third of samples, suggesting growing resistance to this type of disinfectant.
Why soaking the sink works better than a quick flush
The way disinfectants were used mattered as much as which chemical was chosen. The simple rinsing method, even when done twice daily, mainly washed away free-floating bacteria and had little impact on the entrenched biofilm in hidden parts of the sink. After 24 hours, contamination frequently bounced back, with two-thirds of sinks again testing positive in some groups. In contrast, the 30‑minute soaking method allowed the disinfectant—especially the chlorine solution—to seep into the biofilm and break it down. In this setup, no P. aeruginosa was detected right after cleaning, and only a small fraction of sites showed regrowth after a day. The slow-release soaking method, which specifically targeted the U-shaped trap where biofilms concentrate, was also effective but more complicated to run and required special equipment.
Turning results into practical sink care
From a day-to-day hospital operations standpoint, the chlorine soaking method balanced strong germ killing, lasting protection, and ease of use. Staff could apply it early in the morning, when sinks were used less, without major disruption. While high-strength chlorine can corrode metal over time and may encourage resistance genes if misused, the concentration and contact time tested here were both effective and practical. The findings suggest that hospitals should not rely on quick rinses or weaker disinfectants alone. Instead, regularly soaking sinks and traps with an appropriate chlorine solution can substantially reduce hidden colonies of P. aeruginosa. For patients and families, the takeaway is reassuring: thoughtful sink design and smarter cleaning protocols can turn a quiet reservoir of dangerous germs into a far safer part of the care environment.
Citation: Dan, L., Yanni, W., Guiyi, L. et al. Evaluation of disinfection methods and effects for handwashing sinks contaminated with Pseudomonas aeruginosa. Sci Rep 16, 6046 (2026). https://doi.org/10.1038/s41598-026-36670-4
Keywords: hospital sink disinfection, Pseudomonas aeruginosa, healthcare-associated infection, biofilm in drains, chlorine-based cleaners