Clear Sky Science · en
Cardiovascular disease prevention by personalized health promotion considering educational attainment
Why schooling matters for heart health
Heart disease is still the world’s top killer, but many heart attacks and strokes can be delayed or avoided with healthier habits. This study asks a deceptively simple question with big real‑life consequences: when people receive personalized lifestyle advice to protect their hearts, do those with more years of schooling actually benefit more than those with less? And does this difference look the same in women and men?

Personal advice for everyday habits
Researchers in Girona, a region in northeastern Spain, invited adults aged 35 to 74 with no history of cardiovascular disease to take part in a year‑long trial. All 759 participants had their weight, blood pressure, blood fats, blood sugar, diet and physical activity measured at the start and again 12 months later. Half were randomly assigned to an intervention group that received tailored recommendations on eating, exercise, weight control and smoking, based on each person’s measured risk. A trained nurse spent about half an hour explaining this guidance one‑on‑one. The other half formed a control group and received only a standard summary letter of their baseline results by mail.
Schooling levels and starting point
The team focused on people’s highest level of education, grouping them into lower educational attainment (no formal, primary or secondary schooling) or higher educational attainment (university). At the start of the study, participants with less schooling already had a less favorable heart‑health profile: on average they had higher blood pressure and worse cholesterol levels than those with university education. These gaps were more pronounced in women, who were also more likely than men to belong to the lower‑education group. Because both age and sex strongly shape heart‑disease risk, the analyses were adjusted for age and examined women and men separately.
Who improved most over 12 months?
The researchers then asked whether education level changed how well the personalized advice worked. They looked at changes in several measures over the year: upper and lower blood pressure, “bad” LDL cholesterol, “good” HDL cholesterol, blood sugar, body mass index, adherence to a Mediterranean‑style diet and calories burned in leisure‑time physical activity. Among men, schooling did not meaningfully alter the impact of the intervention: improvements, where they occurred, were similar in those with higher and lower education, and differences between groups were small. In the control men, education also did not clearly change trajectories over time.
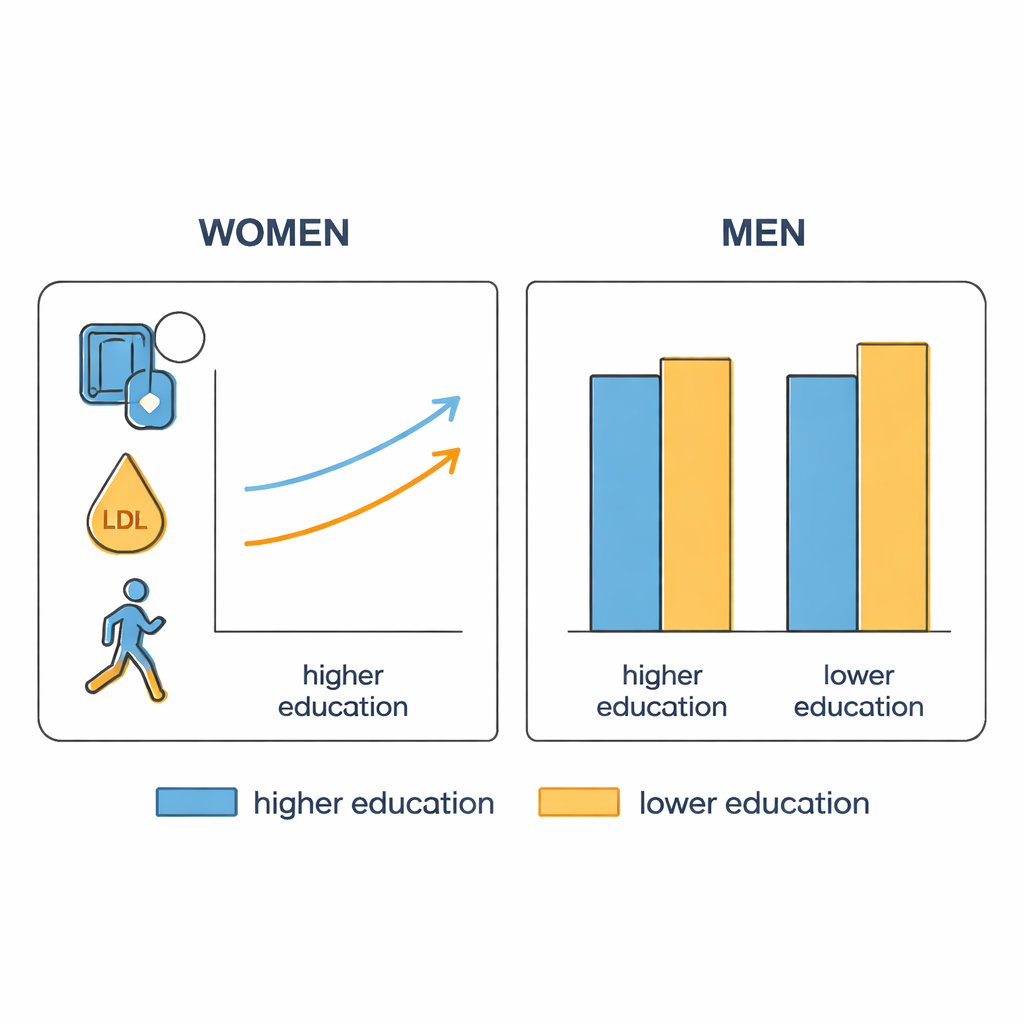
A sharper divide among women
For women, the picture was different. Women with university education who received personalized advice tended to show more favorable 12‑month changes in lower (diastolic) blood pressure, LDL cholesterol and energy spent in physical activity than women with less schooling. In contrast, women with lower educational attainment in the intervention group showed little or even slightly worse change in these same measures. Statistical tests suggested that, in women only, education significantly modified how the intervention affected lower blood pressure and LDL cholesterol, and showed a borderline effect for physical activity. Yet it is important to note that overall shifts within each group were modest, and many did not reach the customary thresholds for statistical certainty.
What this means for real‑world prevention
To a layperson, the takeaway is that giving everyone the same individualized lifestyle advice does not guarantee the same benefits for everyone. In this study, better‑educated women appeared to make more heart‑healthy gains from the guidance, while women with less schooling—who already faced higher risk—benefited less. Men showed fewer differences by education. These findings suggest that successful heart‑disease prevention must look beyond blood tests and blood‑pressure readings to also address schooling, health literacy and social conditions. Programs may need clearer communication, extra support and gender‑sensitive design to ensure that people with fewer educational opportunities are not left behind in the push for healthier hearts.
Citation: Zomeño, M.D., Álamo-Junquera, D., Pericas, C. et al. Cardiovascular disease prevention by personalized health promotion considering educational attainment. Sci Rep 16, 6604 (2026). https://doi.org/10.1038/s41598-026-36654-4
Keywords: cardiovascular prevention, health literacy, educational attainment, personalized lifestyle advice, women’s heart health