Clear Sky Science · en
Advanced oxidation protein products and ischemia-modified albumin as prognostic biomarkers of long-term mortality in community-acquired pneumonia: a prospective observational study
Why pneumonia patients need better warning signs
Community‑acquired pneumonia is a common lung infection that can send otherwise independent adults to the hospital and, in many cases, prove fatal weeks or even months later. Doctors can usually tell who is sick enough to need admission, but they are less good at spotting which patients, once treated and discharged, still carry a high risk of dying. This study asks whether simple blood tests that reflect "rust" inside the body—damage caused by oxygen‑based chemicals—could help flag pneumonia patients who are in deeper trouble than they appear.
Hidden damage from a common lung infection
Pneumonia that starts in the community, rather than in the hospital, affects up to 25 out of every 1,000 people each year and is especially dangerous for older adults and those with other illnesses. Even when antibiotics clear the infection, some patients never fully bounce back. Researchers increasingly suspect that an out‑of‑control inflammatory response and a burst of highly reactive oxygen molecules injure blood vessels and organs far beyond the lungs. In this work, scientists focused on two blood markers that capture this hidden damage: advanced oxidation protein products (AOPPs), which signal proteins that have been chemically scarred, and ischemia‑modified albumin (IMA), a form of the main blood protein that has been altered by lack of oxygen and oxidative stress.
Following pneumonia patients over time
The team enrolled 71 adults hospitalized with community‑acquired pneumonia in Poland, most in their early seventies, and measured AOPPs and IMA in blood samples taken within a day of admission. They also recorded common lab values, such as clotting tests and heart‑related markers, and summarized long‑standing illnesses using a standard comorbidity score. The patients were then followed for 100 days to see who survived. Instead of looking only at immediate complications in the hospital, the researchers deliberately chose this longer window to capture deaths that occur after the apparent crisis has passed.
What the blood markers revealed
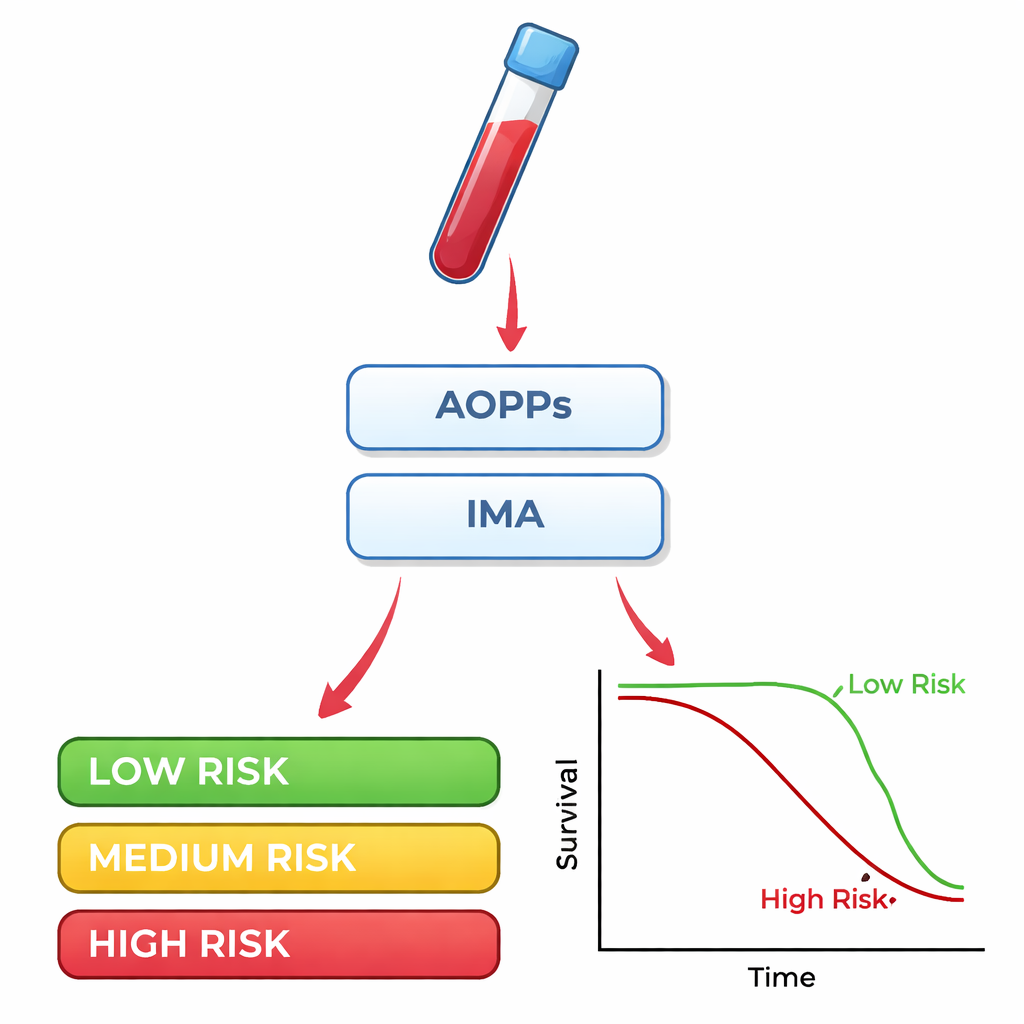
Patients who died within 100 days had clearly higher levels of both AOPPs and IMA when they first arrived at the hospital. Statistical tests showed that these two markers did a fair job of telling survivors from non‑survivors: on a standard accuracy scale from 0.5 (no better than a coin toss) to 1.0 (perfect), each scored around 0.75. When the researchers combined AOPPs and IMA, the accuracy improved, and adding the comorbidity score pushed it higher still. Simple survival curves told a similar story: people whose AOPPs or IMA values were above specific cut‑off points at admission were much more likely to die over the following three months than those below those thresholds. By contrast, two natural antioxidant enzymes often discussed in biology, superoxide dismutase and glutathione peroxidase, were not helpful in predicting outcome.
Links to the heart, blood, and liver
The oxidative stress markers were also tied to subtle signs of strain in other organs. Higher IMA tracked with blood indicators of heart stress and injury, suggesting that the same processes harming the lungs may be putting extra load on the heart. AOPPs rose alongside D‑dimer, a marker of clot formation and breakdown, hinting at disturbed blood clotting and vessel health. IMA was higher when albumin levels and red blood cell measures were lower, patterns often seen in serious inflammation and chronic disease. Together, these connections support the idea that AOPPs and IMA are not isolated curiosities, but are woven into the broader picture of how severe pneumonia affects the whole body.
What this could mean for patients and doctors
The authors conclude that blood tests for AOPPs and IMA, taken as patients enter the hospital, may help identify those with pneumonia who face a higher risk of dying over the next few months, especially when combined with a simple count of their other illnesses. For a layperson, this means that beyond standard scans and routine blood work, there may soon be additional tools to gauge who needs closer monitoring, more aggressive treatment, or careful follow‑up after discharge. Because this was a relatively small, single‑center study, these markers are not ready for everyday use, but they point toward a future in which measuring the body’s internal "oxidative wear and tear" could improve how doctors triage and protect vulnerable pneumonia patients.
Citation: Napiórkowska-Mastalerz, M., Wybranowski, T., Sikora, J. et al. Advanced oxidation protein products and ischemia-modified albumin as prognostic biomarkers of long-term mortality in community-acquired pneumonia: a prospective observational study. Sci Rep 16, 7809 (2026). https://doi.org/10.1038/s41598-026-36643-7
Keywords: community-acquired pneumonia, oxidative stress, biomarkers, AOPPs, ischemia-modified albumin