Clear Sky Science · en
An automatic congenital radio-ulnar synostosis deformity evaluation method (CRUS-DE): integrating TLT-SAM and GPMM-R for landmark identification
Why this matters for kids’ arm surgery
Some children are born with their two forearm bones fused together near the elbow, a condition called congenital radio‑ulnar synostosis. Because the bones cannot rotate properly, simple tasks like turning a doorknob or using utensils can be difficult or impossible. Surgeons can correct the problem with carefully planned bone cuts, but today that planning is often slow and dependent on individual experience. This study introduces a computer method that reads standard CT scans and automatically measures how twisted and bent the bones are, aiming to make treatment more precise, reproducible, and widely available.
When two forearm bones grow as one
In a healthy arm, the radius and ulna act like a pair of parallel rails that can roll around each other, allowing the hand to turn palm‑up and palm‑down. In congenital radio‑ulnar synostosis, part of these bones is fused from birth, usually near the elbow. This locks the forearm in a fixed rotation and often adds extra bends in several directions, limiting daily activities and affecting confidence and social life. Surgeons can perform osteotomy—cutting and realigning bone—to improve function. However, to decide where and how much to cut, they must first quantify the deformity in three dimensions, a task that is extremely hard to do by eye on X‑rays or even CT images. 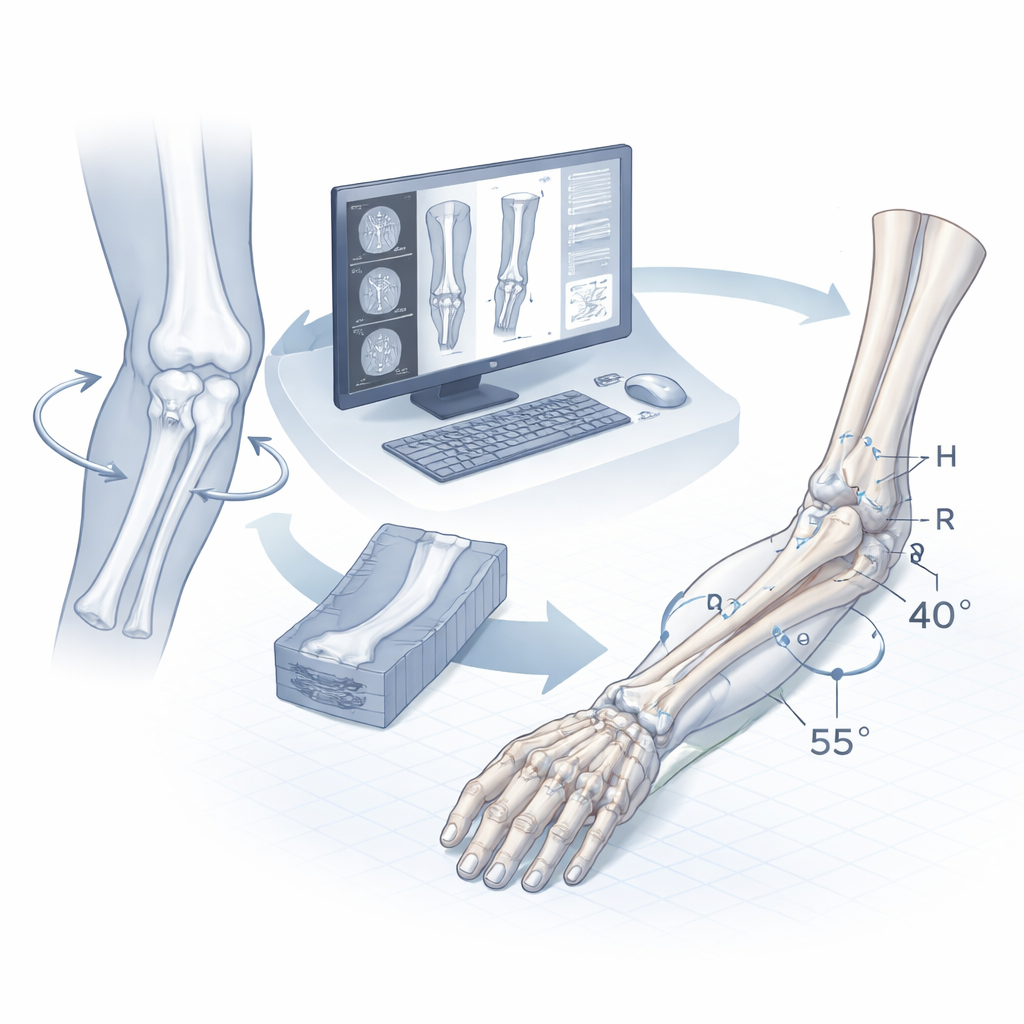
Teaching computers to see children’s bones
The researchers developed a pipeline they call CRUS‑DE that starts from ordinary CT scans of both forearms. First, the system must find the bones and separate them from surrounding tissue. Instead of training a large deep‑learning network, which would require thousands of rare pediatric cases, the team combined a traditional “threshold” method with a modern vision tool known as the Segment Anything Model. Their threshold‑layer tracking follows the bone appearance slice by slice through the scan, while the newer model cleans up and completes the outlines, even where the bone is faint or partially blurred. Tests against careful manual segmentations by a senior surgeon showed that this hybrid approach matched the human outlines very closely.
Locating tiny landmarks on growing bones
Accurate measurements depend on a consistent set of anatomical landmarks: small bumps, tips, and edges on the radius and ulna that define local coordinate systems. In children, these features are often smooth and subtle, and in fused bones they may be distorted or partly missing. To handle this, the authors built statistical “shape templates” of normal pediatric bones using a technique called Gaussian Process Morphable Models. The computer learns how bone shapes typically vary across many healthy children, then gently deforms this template to match each new patient’s bones. From this match it gets preliminary landmark positions, which are then refined using simple geometric rules tailored to anatomy—for example, choosing the most protruding point in a small neighborhood. Across 40 bones, the average distance between automatic and expert‑defined landmarks was about one to one and a half millimeters, with no meaningful differences from manual marking. 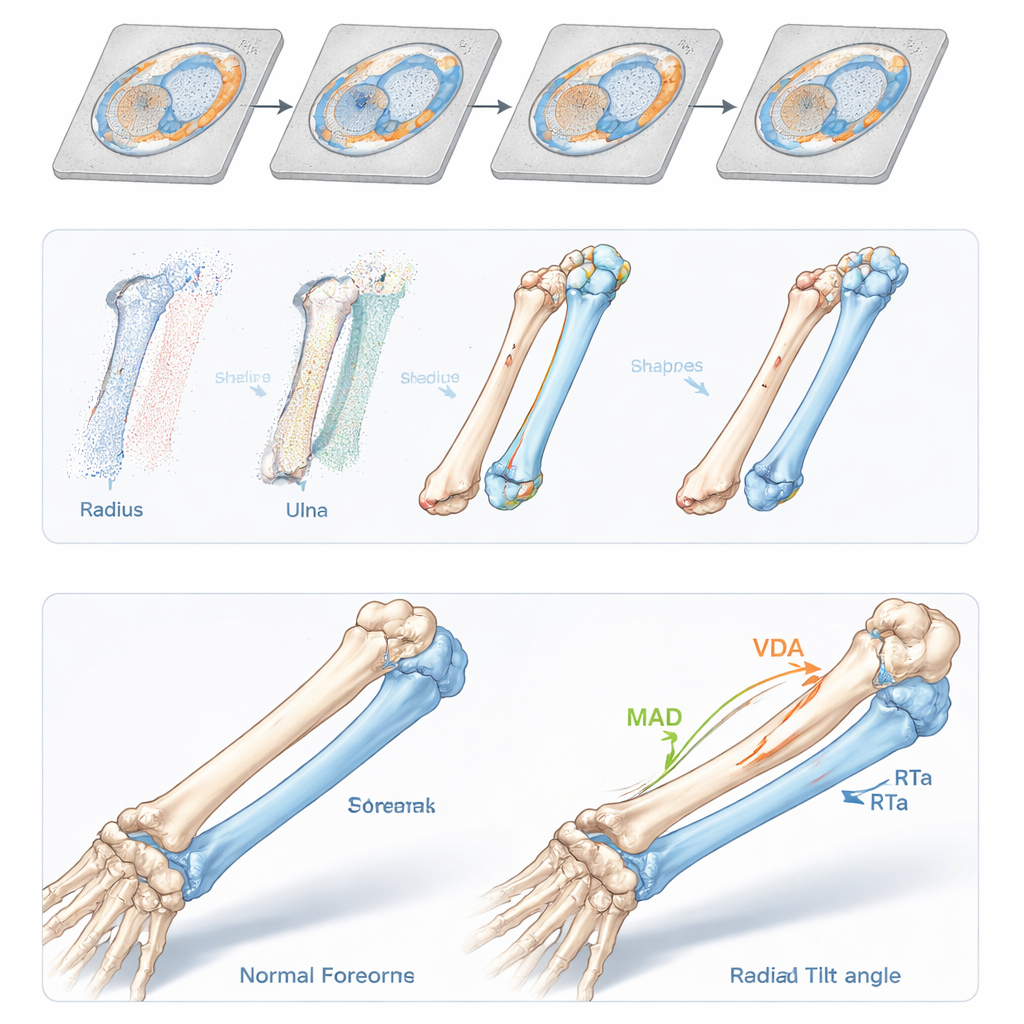
Turning shapes into meaningful angles
With both bones segmented and landmarks identified, CRUS‑DE constructs local coordinate systems at the wrist and elbow. It aligns a patient’s affected forearm with a normal reference and calculates how far the radius and ulna deviate in different directions—toward the thumb or little‑finger side, toward the palm or back of the hand, and how much they are twisted internally. In 40 forearms, including both normal and fused cases, the automatically computed angles differed from expert measurements by less than about 2.5 degrees on average. Importantly, all six measured angles clearly separated normal from CRUS forearms, capturing both the extra bending and the often very large internal rotation that patients experience.
What this could mean for future surgery
For families, the key message is that computers can now help surgeons describe a child’s forearm deformity in precise, objective numbers rather than rough visual impressions. This method turns CT data into a 3D model with highlighted landmarks and quantified angles that show exactly how the bones are misaligned. Such information can guide preoperative planning, help less‑experienced surgeons achieve results similar to experts, and make it easier to evaluate how well surgery has corrected the problem afterward. The authors also envision combining these automatic measurements with custom cutting guides and robotic tools, potentially leading to safer, more accurate, and more personalized operations for children born with this challenging condition.
Citation: Liu, L., Cui, Y., Zhou, T. et al. An automatic congenital radio-ulnar synostosis deformity evaluation method (CRUS-DE): integrating TLT-SAM and GPMM-R for landmark identification. Sci Rep 16, 6434 (2026). https://doi.org/10.1038/s41598-026-36638-4
Keywords: congenital radio-ulnar synostosis, forearm deformity, osteotomy planning, medical image analysis, pediatric orthopedics