Clear Sky Science · en
Clinical relevance of partial HPV genotyping in cervical cancer screening
Why this matters for women’s health
Cervical cancer is one of the most preventable cancers, yet thousands of women worldwide are still diagnosed every year. Modern screening increasingly relies on tests for human papillomavirus (HPV), the virus that causes nearly all cervical cancers. This study from Finland asks a practical question with real-life consequences: if doctors look not just for HPV in general, but specifically for its riskiest types—HPV16 and HPV18—can they better decide which women need closer follow-up and which can safely avoid extra tests?
A closer look at HPV types
HPV is not a single virus but a large family of related types. A small group, called high-risk HPV, is linked to cervical cancer. Even within this high-risk group, some types are more dangerous than others. HPV16 and HPV18 are known worldwide as the biggest culprits. Finland’s national screening program has used HPV testing since 2012, but until now, it has treated all high-risk HPV types the same in how it manages patients. The authors studied whether separating HPV16 and HPV18 from the other high-risk types could sharpen risk estimates and improve how women are triaged after a positive test.
Following more than 76,000 screened women
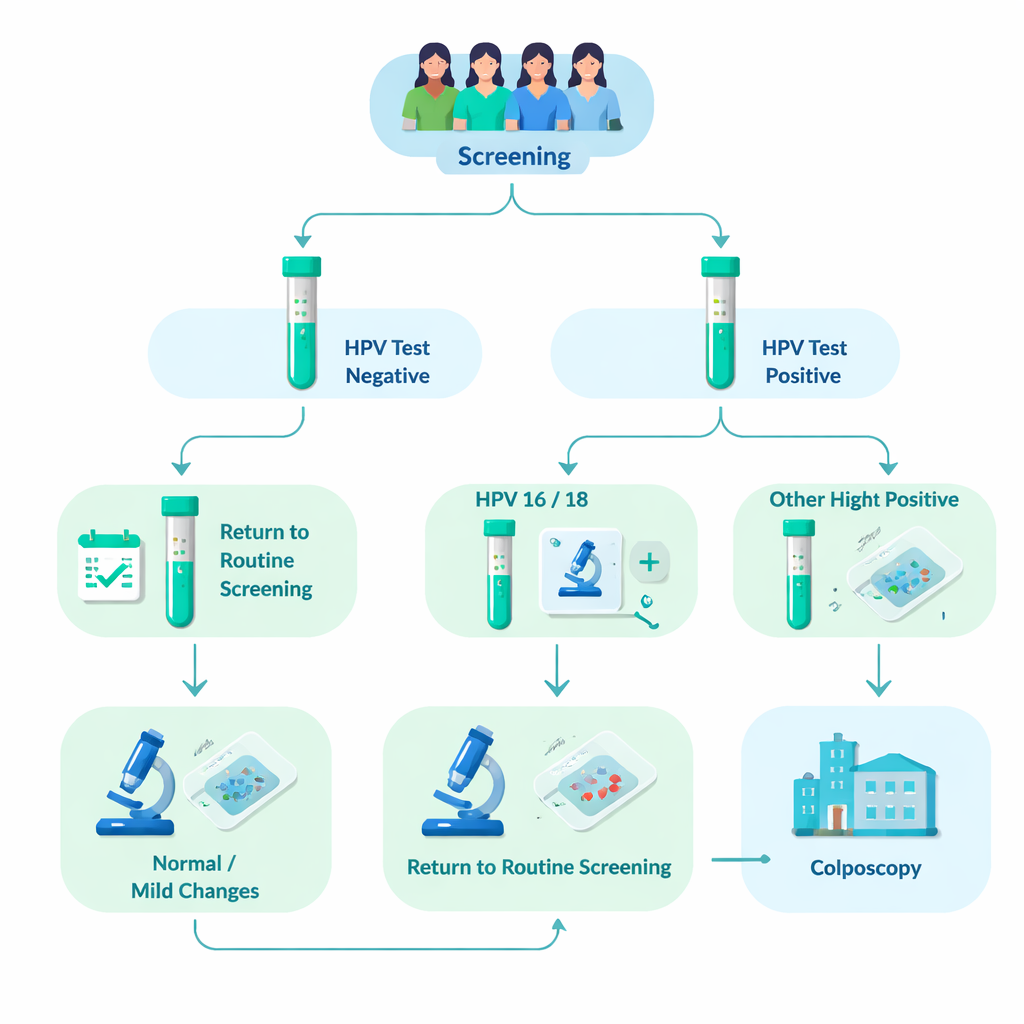
The research team analyzed data from 76,482 women who attended organized cervical screening in Tampere and nearby municipalities between 2012 and 2023. About 8% (6031 women) tested positive for high-risk HPV. All of these women had an additional microscope exam of their cervical cells (cytology). Those whose cell samples already showed clear abnormalities were sent directly to a closer examination called colposcopy, where small tissue samples (biopsies) could be taken. Women whose cell samples looked normal or only mildly abnormal were asked to return in 12–24 months for a repeat HPV test. If HPV persisted, they too were referred to colposcopy. This real-world design allowed the researchers to see how often serious tissue changes actually appeared in each HPV genotype group over several years.
Risk is not the same for all high-risk HPV
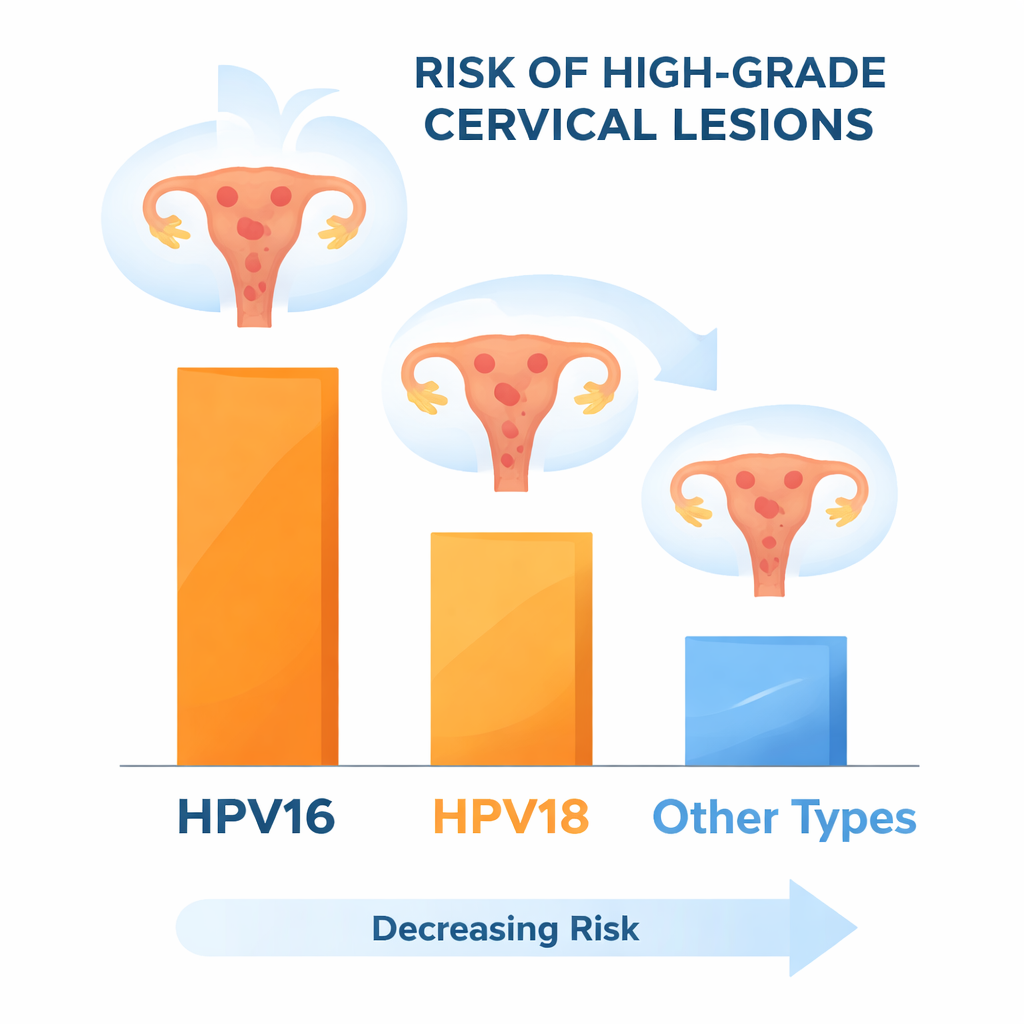
When the team compared outcomes, HPV16 clearly stood out. Among women who were HPV-positive, serious tissue changes—known as high-grade lesions or worse—were found in about 37% of those with HPV16, 26% of those with HPV18, and only about 20% of women carrying other high-risk types. The risk was especially high for women with HPV16 plus another high-risk type. Younger women (ages 30–40) had more high-grade findings than older women, and HPV16 and HPV18 were more common in these younger age groups. Importantly, even when the initial cell sample looked normal, women with HPV16 or HPV18 still had a much higher chance of having hidden high-grade disease than women with other HPV types.
Persistent infections and what they mean
The study also looked at what happened to women with mild or normal cytology who returned for repeat testing. Among those who initially had HPV16, roughly two-thirds still had the same infection at the follow-up visit, a higher persistence than most other types. Persistent HPV16 or HPV18 infection was often followed by high-grade changes in the cervix. The researchers then asked a “what if?” question: what if all women with HPV16 or HPV18 and mild cytology had been sent straight to colposcopy from the start? They found this would have increased colposcopy referrals by about 7% but would have led to earlier detection of only one invasive cancer case in this cohort—suggesting that the biggest benefit would be streamlining care by skipping an extra repeat test rather than dramatically changing cancer outcomes.
What this means for screening programs
Overall, the findings support using partial HPV genotyping—separating HPV16 and HPV18 from other high-risk types—in Finland’s cervical cancer screening program. Women with HPV16 or HPV18 clearly carry a higher risk and could reasonably be referred directly to colposcopy, even when their cell sample appears normal or only mildly abnormal, especially in younger age groups. This would simplify follow-up, reduce the number of repeat tests, and focus intensive checks on those at greatest risk, while accepting a modest rise in invasive examinations. As HPV vaccination continues to reduce HPV16 and HPV18 in the population, the study also suggests that future screening may need to pay closer attention to other high-risk types. For now, though, using targeted genotyping offers a practical way to make cervical cancer screening both safer and more efficient.
Citation: Leino, A., Numminen, E., Kares, S. et al. Clinical relevance of partial HPV genotyping in cervical cancer screening. Sci Rep 16, 7204 (2026). https://doi.org/10.1038/s41598-026-36594-z
Keywords: HPV16, cervical cancer screening, HPV genotyping, colposcopy, HPV vaccination