Clear Sky Science · en
Evaluation of salivary interleukin 6 interleukin 1 beta and interferon gamma in oral and mucocutaneous lichen planus patients
Why saliva can tell a bigger health story
Most of us think of saliva as just spit, but it actually carries a rich mix of molecules from our blood and tissues. This study explores how simple saliva samples can reveal what is happening in a stubborn inflammatory disease called lichen planus, which can cause painful sores in the mouth and itchy rashes on the skin. By tracking tiny immune signals in spit, the researchers ask whether we could one day monitor this disease—and perhaps tailor treatment—without needles or biopsies.
Two faces of the same illness
Lichen planus is an immune-related condition that attacks the body’s own lining tissues. When it affects only the mouth, it is called oral lichen planus; when it involves both skin and mouth, it is known as mucocutaneous lichen planus. The mouth form can cause white lace-like streaks, burning, and sometimes raw, erosive sores. The mucocutaneous form adds itchy, violet-colored bumps on the skin. Because long-lasting mouth lesions may have a small risk of turning cancerous, doctors are eager for better ways to track which patients have more active disease and need closer follow-up.
Testing spit instead of drawing blood
To probe the immune activity behind these conditions, the team in Iraq enrolled 60 adults: 20 healthy volunteers, 20 people with oral lichen planus, and 20 with mucocutaneous lichen planus. All patients had their diagnoses confirmed by both clinical exam and tissue analysis. Participants provided unstimulated saliva in the morning after avoiding food and drink, and the samples were processed and frozen for testing. Using a laboratory technique called ELISA, the researchers measured three immune messenger proteins—interleukin‑6, interleukin‑1 beta, and interferon‑gamma—that are known to drive inflammation. For the mouth-only group, they also scored how widespread and severe the oral lesions were, using a standardized system that considers white streaks, redness, and ulcers.
Stronger immune signals in patient saliva
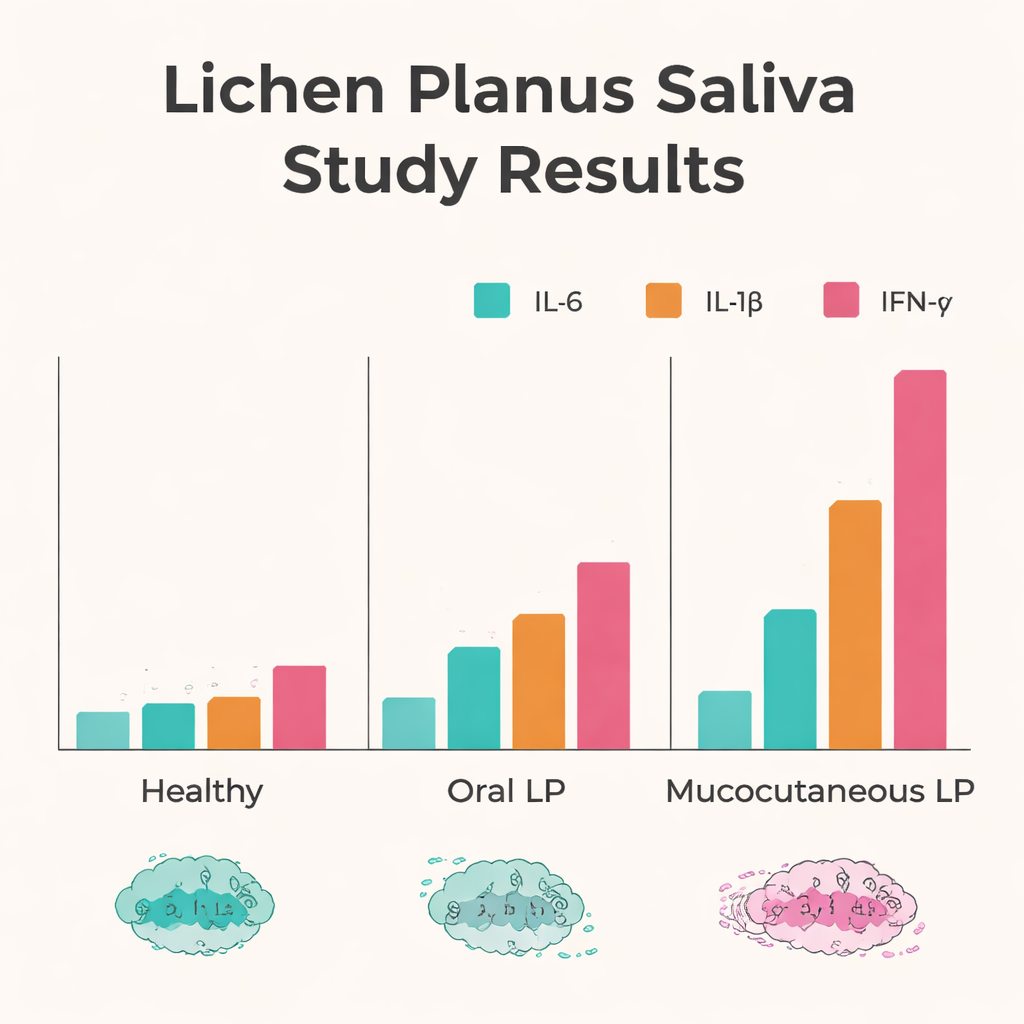
The results showed a clear pattern: all three immune messengers were higher in patients than in healthy people. Levels of interleukin‑6 in saliva were about five to six times higher in both oral and mucocutaneous lichen planus than in controls. Interleukin‑1 beta was roughly doubled in both patient groups. Interferon‑gamma showed the most dramatic change, rising about threefold in patients overall—and it was highest in those with both skin and oral disease. When the researchers compared two common mouth patterns, they found that the more aggressive erosive form carried higher levels of interleukin‑1 beta and interferon‑gamma than the milder lace-like reticular form, hinting that these molecules track with more damaging inflammation.
Linking saliva markers to symptom burden
Beyond simple group differences, the study looked at how saliva readings related to the visible severity of mouth lesions. In people with oral lichen planus, higher interleukin‑6 levels went hand in hand with more severe and widespread oral damage. This suggests that interleukin‑6 could act as a rough gauge of how active the disease is in the mouth. In contrast, among those with mucocutaneous disease, interleukin‑1 beta showed a negative relationship with oral severity, implying that the broader body-wide immune picture may differ when the skin is involved. Interestingly, interferon‑gamma—despite being strongly elevated overall—did not closely track with how bad the mouth lesions looked, especially in the combined skin-and-mouth form.
What it could mean for future care
Taken together, these findings paint saliva as a promising, needle-free window into the hidden immune storms driving lichen planus. The clear separation between patients and healthy volunteers suggests that a small saliva sample might help confirm a diagnosis or flag ongoing inflammation. The tighter link between interleukin‑6 and oral disease severity points to this molecule as a potential marker for monitoring flares in mouth-only cases, while especially high interferon‑gamma levels in people with skin involvement hint at a broader, more intense immune activation. Although this single-center study is relatively small and captures only one moment in time, it supports the idea that customized treatment and follow-up might someday be guided by simple saliva tests, making care less invasive and more closely matched to each patient’s underlying biology.
Citation: Hama, P.N., Ahmed, K.M. Evaluation of salivary interleukin 6 interleukin 1 beta and interferon gamma in oral and mucocutaneous lichen planus patients. Sci Rep 16, 5678 (2026). https://doi.org/10.1038/s41598-026-36506-1
Keywords: oral lichen planus, mucocutaneous lichen planus, salivary biomarkers, cytokines, interleukin-6