Clear Sky Science · en
Classification of temporomandibular joint hypermobility based on lateral TMJ, and magnetic resonance imaging contributing to a nonsurgical treatment protocol
Why jaw joint “over-flexibility” matters
Many people can open their mouths wide enough to bite a tall sandwich or yawn deeply without thinking about it. But for some, the jaw joint at the side of the face – the temporomandibular joint, or TMJ – moves too far and too freely. This can lead to painful popping, the jaw getting stuck open, or a constant fear that a big yawn will send them to the emergency room. The study summarized here set out to bring order to this confusing problem by creating a simple, image-based way to sort different types of jaw over‑movement and to match each type with a non‑surgical treatment plan.
Turning scattered symptoms into clear stages
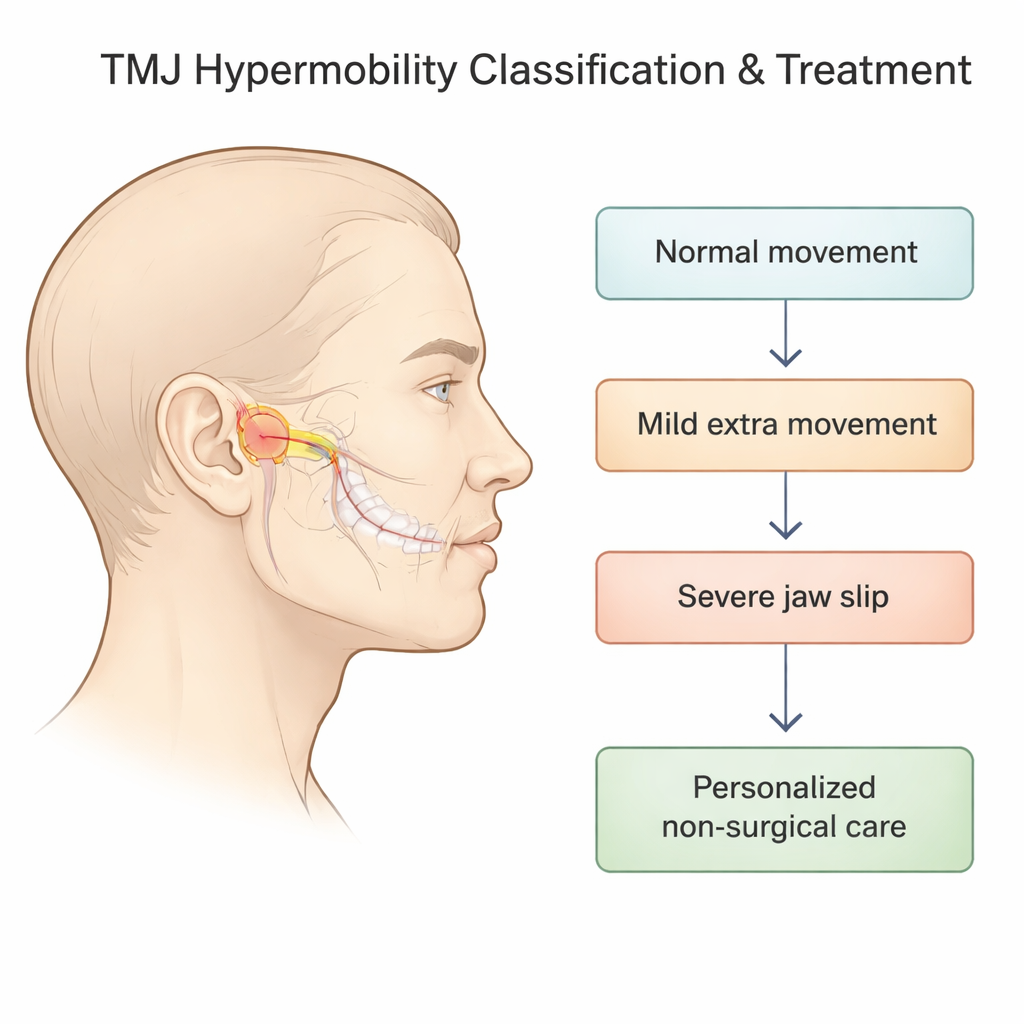
The researchers focused on TMJ “hypermobility” – situations where the moving part of the jaw joint (the condyle) slides too far forward out of its socket and may drag or lose the cushioning disk that sits between the bones. Earlier systems tried to describe this with X‑rays alone, but they left out what was happening to the disk and did not always reflect how the jaw actually felt and functioned. In this project, the team combined side‑view X‑rays of the joint with MRI scans, which can show the disk and surrounding soft tissue in detail, to build a five‑stage classification that ranges from normal movement to severe, non‑self‑correcting dislocation.
From normal motion to jaw “slip” and lock
In the new system, Stage 0 represents normal opening: the jaw bone ends up directly under the bony ridge in front of the ear, and the disk sits neatly between the bone and socket. Stages 1 and 2 describe “self‑reducing” jaw slips, where the condyle moves in front of the ridge but can still return on its own; within each of these, the disk may be normal, briefly slip forward and pop back, or stay out of place. Stage 3 covers more serious events in which the jaw becomes stuck open and does not go back by itself, while Stage 4 captures a pattern where the disk shifts backward during opening. This fine‑grained view matters because the exact pairing of bone position and disk behavior helps predict symptoms such as clicking, pain, or locking, and suggests how aggressively the joint needs to be stabilized.
Testing a stepwise, needle‑based treatment plan
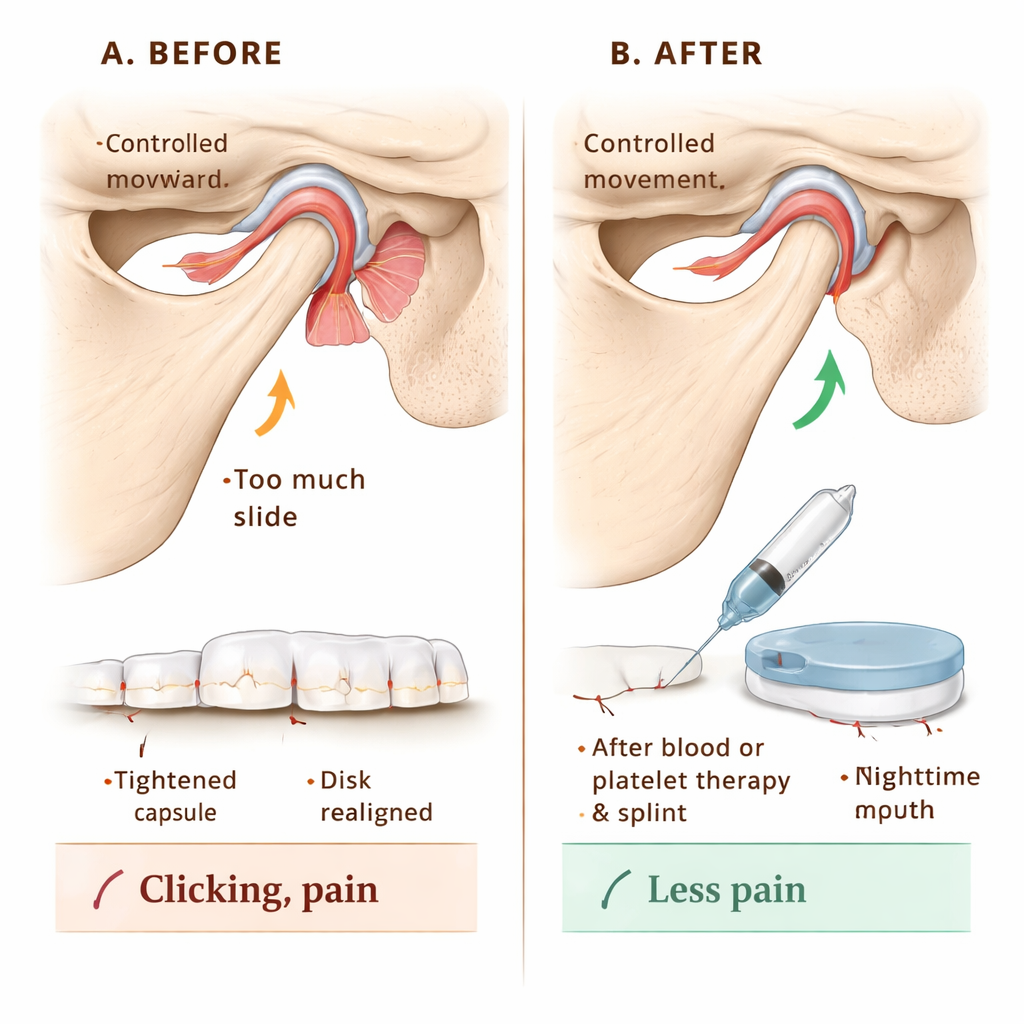
To see if this classification could guide care, the team followed 144 patients with TMJ hypermobility. Everyone received education on protecting the joint – for example, avoiding extreme yawns and contact sports. The main treatment was washing out the joint space with fluid (arthrocentesis) and then injecting either the patient’s own blood or a concentrated, growth‑factor‑rich fraction of their blood called injectable platelet‑rich fibrin (I‑PRF). These injections are designed to trigger mild scarring and strengthening around the joint capsule, limiting how far the jaw can slide forward. For patients whose joint surfaces also showed wear and tear, I‑PRF was favored to support tissue healing; others received simple blood injections. In stages where the disk was out of place, patients also wore a custom night‑time bite splint for a year, adjusted in thickness to gently reposition the jaw and encourage a healthier disk‑bone relationship. Short‑term jaw immobilization with bandages, screws, or braces for two weeks helped the injected tissues heal without being overstretched.
Measuring pain, movement, and noise
Over 12 months, the researchers tracked three practical outcomes: how wide patients could voluntarily open their mouths, how much pain they felt on a 0–10 scale, and whether joint noises such as clicks or pops were present. Before treatment, many patients could open their mouths extremely wide – a sign of over‑movement rather than health – and reported high pain scores around 8 out of 10, with joint sounds in every case. After treatment, average opening narrowed into a more normal range, pain scores fell to zero by six months and stayed there, and joint sounds disappeared in all patients from the first‑month check‑up onward. Blood injections and I‑PRF both worked well; blood alone slightly outperformed I‑PRF in limiting jaw over‑opening, while longer‑term pain relief ended up similar between the two methods.
What this means for people with jaw trouble
For patients and clinicians, this work offers a clearer roadmap. Instead of treating every noisy or unstable jaw the same way, doctors can use simple imaging to assign a stage that captures both how far the jaw bone moves and what the cushioning disk is doing. That stage then points to a tailored, non‑surgical plan that combines education, brief immobilization, targeted joint injections, and, when needed, a carefully designed splint. The results of this study suggest that such an approach can reliably reduce pain, quiet troublesome clicks, and rein in excessive jaw motion without resorting to bone‑altering surgery in most cases.
Citation: Hegab, A.F., Shuman, M., Al Hameed, H.A. et al. Classification of temporomandibular joint hypermobility based on lateral TMJ, and magnetic resonance imaging contributing to a nonsurgical treatment protocol. Sci Rep 16, 6345 (2026). https://doi.org/10.1038/s41598-026-36461-x
Keywords: jaw joint, TMJ hypermobility, MRI, non-surgical treatment, blood injection