Clear Sky Science · en
Baseline characteristics associated with mortality among children living with HIV initiating ART at a rural district HIV clinic of Mozambique
Why this study matters for children’s health
HIV treatment has turned a once-fatal infection into a manageable condition for many adults, but children—especially in rural, low‑income settings—still die at worrying rates. This study from a rural district hospital in southern Mozambique followed more than 1,300 children with HIV who started antiretroviral therapy (ART) between 2002 and 2019. By asking who survived and who did not, the researchers identified which children are most at risk, and what can be changed in clinics and health systems to give them a better chance at life.
Life and death in a rural HIV clinic
At Carmelo Hospital of Chókwè, a referral center serving a largely rural population, 1,341 children under 15 years old began HIV treatment over a 17‑year period. Together, they contributed more than 6,700 “child‑years” of observation—time during which their progress, setbacks, and outcomes were recorded in an electronic medical record system. Overall, about 14% of these children died while on treatment, which translates to 2.8 deaths for every 100 child‑years, a rate similar to other African settings but still far from acceptable. Most children started care as outpatients and had never received HIV drugs before; many, however, already showed signs of advanced infection when they arrived. 
The youngest children face the steepest climb
Age emerged as one of the strongest predictors of survival. Children aged two years or younger at the time they started treatment were more than twice as likely to die as those who began therapy in early adolescence. Young children have less mature immune systems and are more vulnerable to severe infections and malnutrition. The study’s findings support a broader pattern seen across Africa: delays in diagnosing HIV in infants, combined with limited access to good nutrition and preventive medicines, create a dangerous window of time in which even life‑saving ART may come too late to fully reverse the damage.
When late diagnosis meets serious illness
Beyond age, the severity of illness at the moment treatment began was crucial. Children who started ART while sick enough to be hospitalized had almost double the risk of death compared with those who were well enough to be seen as outpatients. Likewise, those who were already in the most advanced stages of HIV disease, or who had very low CD4 cell counts—a marker of a badly weakened immune system—were several times more likely to die. Many of these children were also fighting tuberculosis (TB). If they needed TB treatment within three months of starting HIV drugs, their risk of death nearly doubled, reflecting both the toll of TB itself and the complications that can occur when a recovering immune system suddenly reacts strongly to hidden infections.
Not all treatment regimens are equal
The type of HIV drug combination children received also mattered. Regimens built around stavudine (D4T), an older drug now largely phased out, were linked to a much higher risk of death. In contrast, combinations that included protease inhibitors—stronger, more modern HIV drugs—or zidovudine (ZDV) appeared to protect children, cutting mortality risk substantially compared with some tenofovir‑based regimens. Because the study spans many years in which national treatment guidelines changed, some of this pattern reflects broader improvements in care over time. Still, the message is clear: safer, more potent modern regimens are a key part of keeping children alive, especially when started before HIV has ravaged their immune systems. 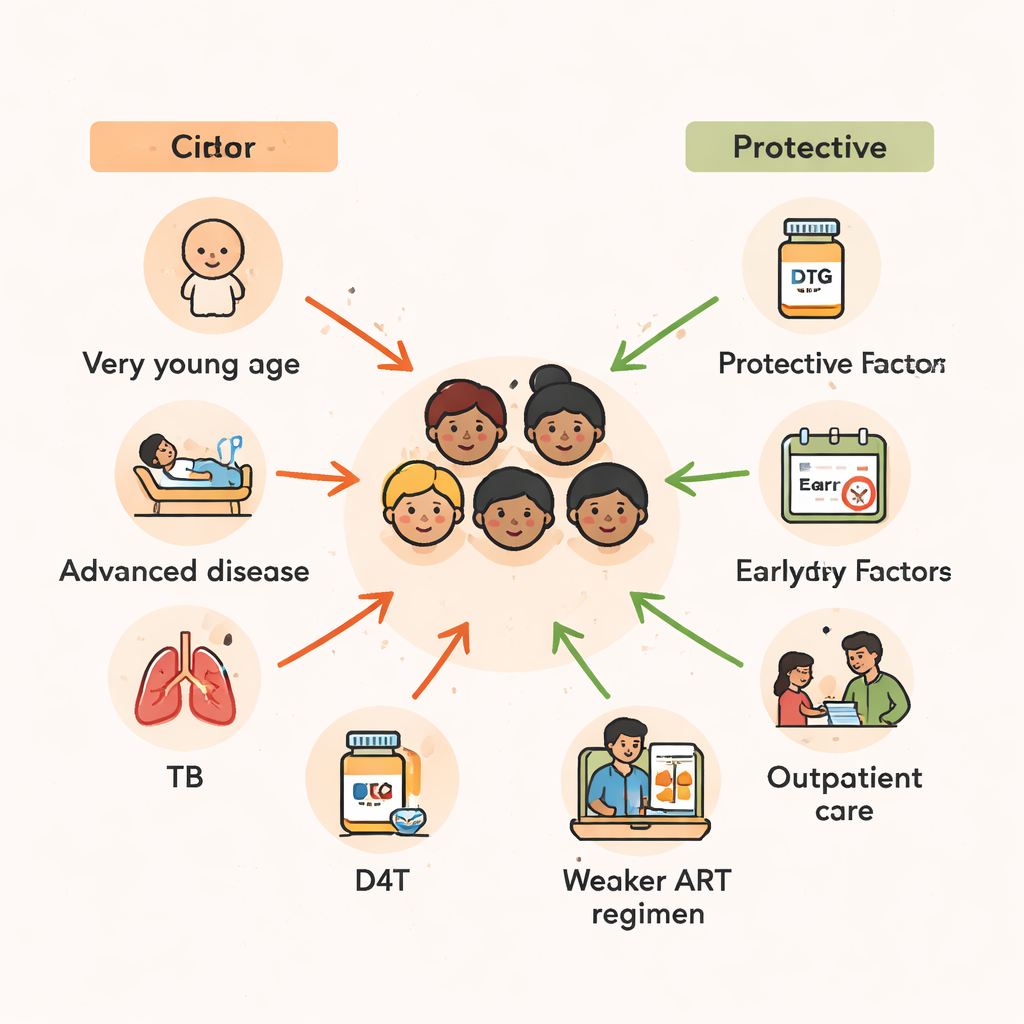
Turning evidence into better care
In plain terms, the study shows that too many children in rural Mozambique are starting HIV treatment late—when they are very young, already very sick, or battling both HIV and TB—and that this delay greatly increases their chances of dying. The authors conclude that to save more lives, clinics must diagnose HIV earlier, especially in infants; start treatment before the immune system collapses; screen carefully for hidden infections like TB; and use the most effective, child‑friendly drug combinations now available, such as those based on protease inhibitors or dolutegravir. Strengthening staff training and family‑centered care in rural areas, they argue, can turn these insights into everyday practice, helping transform HIV from a deadly childhood disease into a controllable one, no matter where a child is born.
Citation: Nacarapa, E., Maddalozzo, R., Moosa, MY.S. et al. Baseline characteristics associated with mortality among children living with HIV initiating ART at a rural district HIV clinic of Mozambique. Sci Rep 16, 6051 (2026). https://doi.org/10.1038/s41598-026-36433-1
Keywords: pediatric HIV, antiretroviral therapy, tuberculosis coinfection, Mozambique, child mortality