Clear Sky Science · en
Utility of prostate-specific antigen derivatives to minimize unnecessary magnetic resonance imaging in patients with prior negative prostate biopsy
Why this matters for men and their families
Prostate cancer is one of the most common cancers in men, and many men undergo painful biopsies and expensive scans to find it. Yet a large number of these tests turn out negative or reveal low‑risk disease. This study explores whether simple blood test measurements, already familiar to many patients as the PSA test, can be used more wisely to decide who really needs a costly MRI scan after a previous negative biopsy—and who can safely skip it.
The challenge of repeated testing
For decades, doctors have relied on the prostate‑specific antigen (PSA) blood test and tissue sampling, called prostate biopsy, to look for cancer. However, standard biopsies can miss tumors, with false‑negative rates reaching up to 40%. Men whose first biopsy is negative but who still have elevated PSA levels often face a difficult choice: undergo more biopsies and high‑tech MRI scans, or wait and worry. While MRI has improved the ability to find important cancers, scanning everyone with a prior negative biopsy is expensive and may not always change outcomes, especially in men whose overall risk of dying from prostate cancer is low.
Looking deeper at PSA numbers
The researchers studied 251 men from a single hospital who had at least one previous negative prostate biopsy, then later had blood tests and MRI before another biopsy. Instead of looking only at the basic PSA value, they examined PSA "derivatives": PSA density (which accounts for prostate size) and the free‑to‑total PSA ratio, which reflects how PSA circulates in the blood. They then compared these numbers with detailed MRI scores called PI‑RADS, which rate how suspicious an MRI lesion is for clinically significant cancer—defined here as a Gleason score of 7 or higher, the level most likely to affect a man’s health and longevity.
Finding practical cutoffs
Using statistical tools known as receiver operating characteristic curves, the team identified an MRI score of PI‑RADS 4 or higher as the most reliable threshold for signaling significant cancer. Next, they asked which PSA‑based values best predicted these high‑suspicion MRI findings. They found that a PSA level of 11.87 ng/mL, a PSA density of 0.19 ng/mL², and a free‑to‑total PSA ratio of 18.76% were useful cutoffs. Among these, PSA density stood out as the strongest single marker. Men who were older and had higher PSA density were more likely to have worrisome MRI findings and clinically significant cancers on targeted biopsy.
Balancing fewer scans with missed cancers
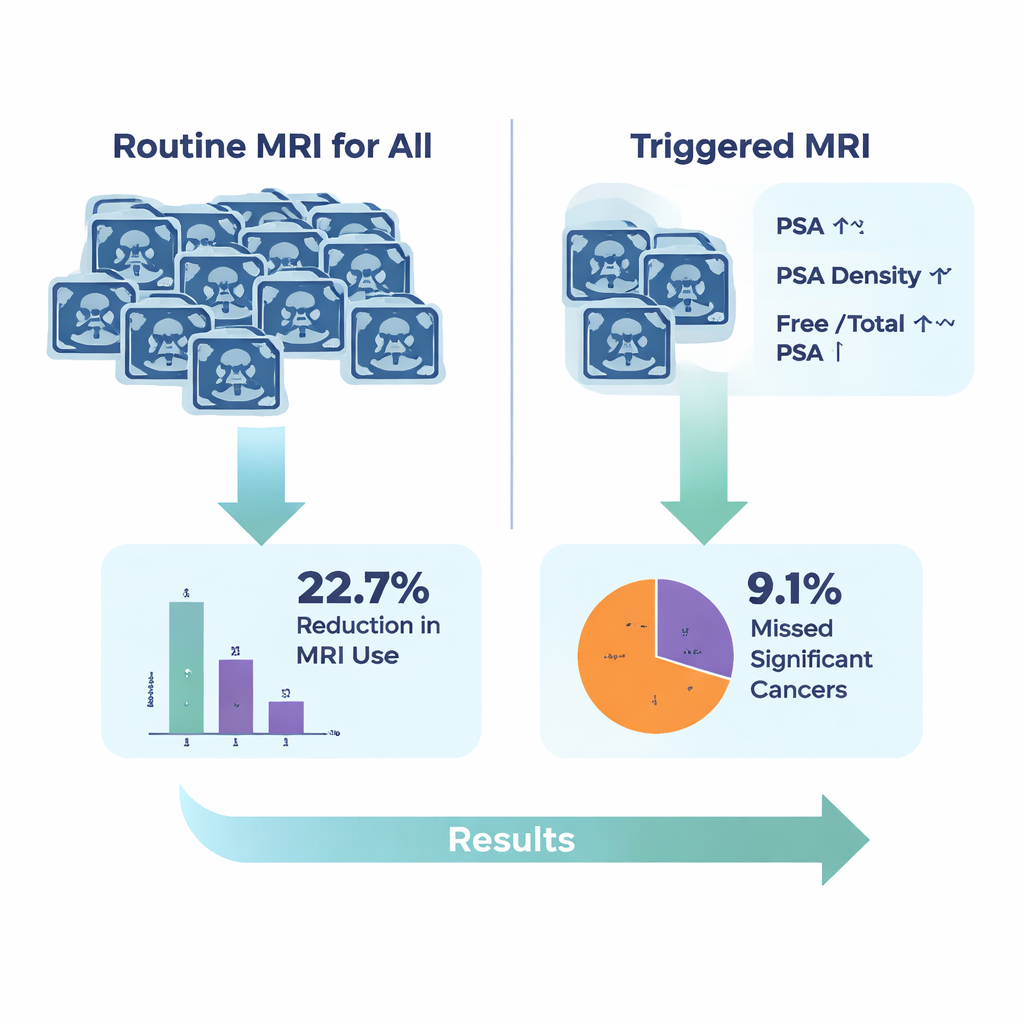
The key question was how much MRI use could be safely reduced by relying on these blood test thresholds. If MRI were avoided in men whose PSA was below 11.87 ng/mL, almost half of all MRIs could be spared—but more than half of significant cancers detected by MRI‑targeted biopsy would be missed, an unacceptable tradeoff. Using PSA density alone would still skip nearly a third of important cancers. However, when the researchers combined all three measures—recommending MRI only when PSA was at least 11.87 ng/mL, PSA density at least 0.19 ng/mL², or the free‑to‑total PSA ratio at or below 18.76%—MRI use could be reduced by about 22.7%, while only 9.1% of significant cancers found by MRI‑targeted biopsy would be missed.
What this means in everyday terms
For men who have already endured a negative prostate biopsy, this study suggests that a more refined reading of familiar blood tests could help avoid nearly a quarter of follow‑up MRI scans, with only a small risk of overlooking serious cancers. The authors emphasize that these cutoffs should not be followed blindly. Instead, they should be combined with newer biomarkers, evolving biopsy techniques, and each patient’s preferences and overall health. Still, the work points toward a future in which men and their doctors can use smarter blood‑based rules to decide who truly needs another scan—and who can safely watch and wait.
Citation: Lee, S., Ryu, H., Song, S.H. et al. Utility of prostate-specific antigen derivatives to minimize unnecessary magnetic resonance imaging in patients with prior negative prostate biopsy. Sci Rep 16, 5202 (2026). https://doi.org/10.1038/s41598-026-36242-6
Keywords: prostate cancer, PSA density, MRI triage, negative prostate biopsy, cancer screening