Clear Sky Science · en
Higher lymph node burden predicts greater chemotherapy benefit in resected pancreatic ductal adenocarcinoma: evidence from 22,045 patients
Why lymph nodes matter after pancreatic cancer surgery
For people facing pancreatic cancer, surgery followed by chemotherapy is often the best hope for longer life. But not every patient responds the same way, and many are too frail after surgery to complete months of additional treatment. This study asks a practical, patient-centered question: among people whose pancreatic tumors have been removed, who stands to gain the most from going through chemotherapy—and can a simple measure taken from the pathology report, the number of cancerous lymph nodes, guide those decisions?
Looking at thousands of real-world patients
The researchers drew on the large U.S. Surveillance, Epidemiology, and End Results (SEER) cancer registry to track 22,045 people with pancreatic ductal adenocarcinoma, the most common and deadly form of pancreatic cancer. All had surgery to remove their tumors and had no distant metastases at the time of diagnosis. Doctors had also recorded how many nearby lymph nodes contained cancer cells. Using the current staging system, patients were grouped into three categories: N0 (no positive nodes), N1 (1–3 positive nodes), and N2 (4 or more positive nodes). About three-quarters of patients received chemotherapy after surgery, while the rest had surgery alone.
How chemotherapy and lymph nodes together shape survival
When the team analyzed survival, two factors stood out above all others: whether patients received chemotherapy and how many lymph nodes were involved. Skipping chemotherapy raised the risk of dying from pancreatic cancer by roughly 70 percent compared with receiving it. Having cancer in the lymph nodes further worsened outcomes in a graded way: people with N1 disease had about a 50 percent higher risk of death than those with N0, and those with N2 disease had more than double the risk. Yet the key insight was not just that both factors were important, but that they worked together in a powerful way—the more lymph nodes involved, the more extra benefit patients seemed to gain from chemotherapy.
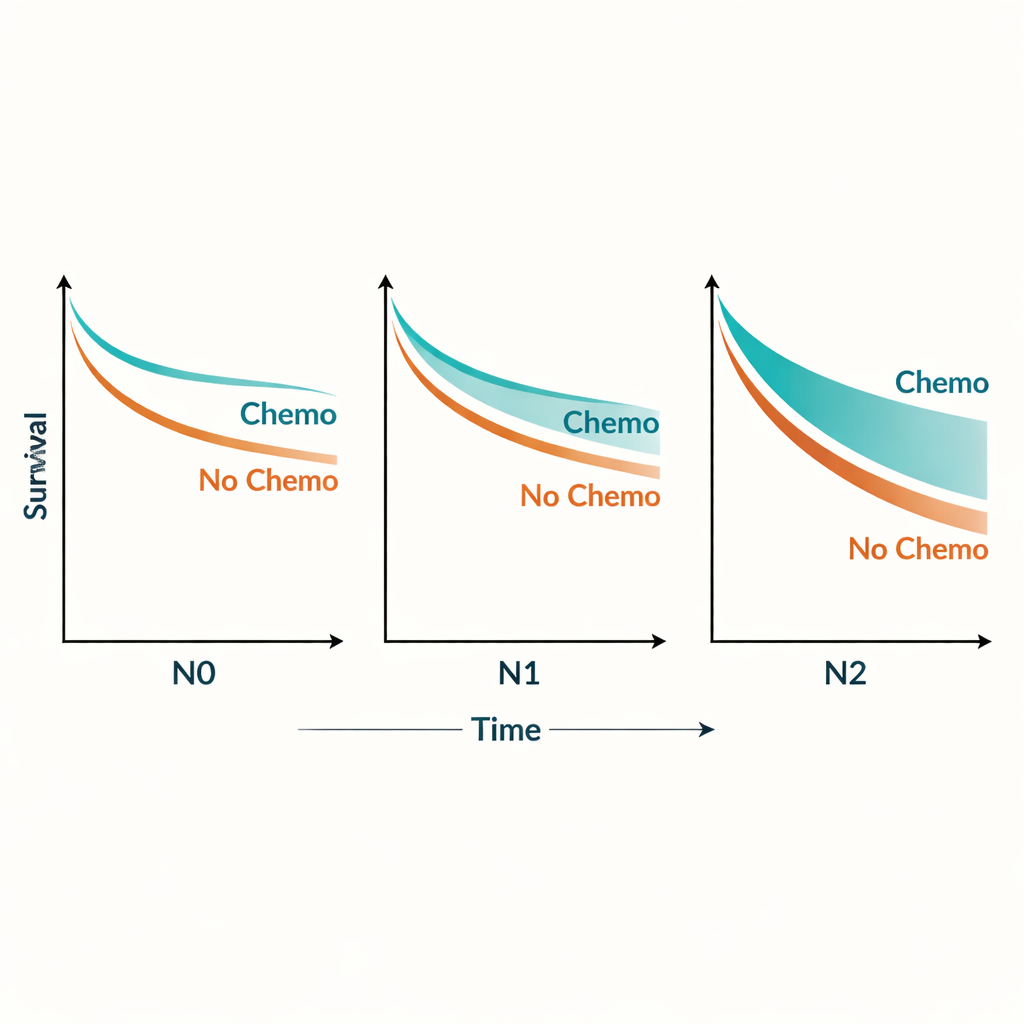
More affected nodes, more to gain from treatment
To explore this pattern, the researchers examined chemotherapy benefit across the full range of positive lymph node counts. They found that the advantage of chemotherapy grew as nodal burden increased and then leveled off once patients reached four or more affected nodes. In practical terms, chemotherapy improved three-year, cancer-specific survival from about 39 to 55 percent in N0 patients, from 18 to 37 percent in N1 patients, and from 9 to 26 percent in N2 patients. Strikingly, people with N1 disease who did receive chemotherapy actually lived longer, on average, than node-negative patients who did not. Even patients with the heaviest lymph node involvement (N2) fared better with chemotherapy than untreated patients with only moderate nodal spread (N1).
Testing the finding from every angle
Because treatment and survival can be influenced by many other factors, the investigators used several layers of statistical checks. They adjusted for age, sex, tumor size and grade, type of surgery, radiation, and socioeconomic variables. They repeated the analyses while accounting for deaths from causes other than cancer, excluded patients who had chemotherapy before surgery, and looked not just at the raw number of positive nodes but also at the proportion of nodes involved. They further tested whether the results held in men and women separately and in patients who had more or fewer lymph nodes examined by the surgeon and pathologist. Across all of these alternate views, the same pattern emerged: higher lymph node burden consistently marked patients who obtained a disproportionately greater survival boost from chemotherapy.
What this means for patients and doctors
For someone recovering from pancreatic cancer surgery, the decision to pursue chemotherapy can be daunting, especially when complications or fatigue make treatment hard to complete. This study suggests that the number of cancerous lymph nodes in the surgical specimen could be used as a simple, widely available guide to how much benefit chemotherapy is likely to bring. Patients with N1 or N2 disease—those whose cancer has already reached multiple nearby nodes—appear to gain the most additional survival from chemotherapy and may warrant extra support to start treatment promptly and see it through. While chemotherapy remains beneficial even for patients without lymph node involvement, lymph node status emerges here not just as a marker of how aggressive the cancer is, but as a signal of who may benefit most from intensive post-surgical therapy.
Citation: Zhou, J., Dou, X., Wei, W. et al. Higher lymph node burden predicts greater chemotherapy benefit in resected pancreatic ductal adenocarcinoma: evidence from 22,045 patients. Sci Rep 16, 7227 (2026). https://doi.org/10.1038/s41598-026-36035-x
Keywords: pancreatic cancer, lymph nodes, chemotherapy, survival benefit, risk stratification