Clear Sky Science · en
Lactate to albumin ratio predicts one year mortality in ICU patients receiving invasive mechanical ventilation
Why this matters for people in intensive care
When a loved one is placed on a breathing machine in an intensive care unit (ICU), families desperately want to know what to expect. Doctors use complex scoring systems and dozens of measurements to estimate the chances of survival, but these tools can be hard to apply and sometimes give uncertain answers. This study explored whether a simple ratio of two routine blood tests—the lactate‑to‑albumin ratio, or LAR—can help identify which ICU patients on invasive mechanical ventilation are at higher risk of dying within the next year.
A simple signal hidden in routine blood tests
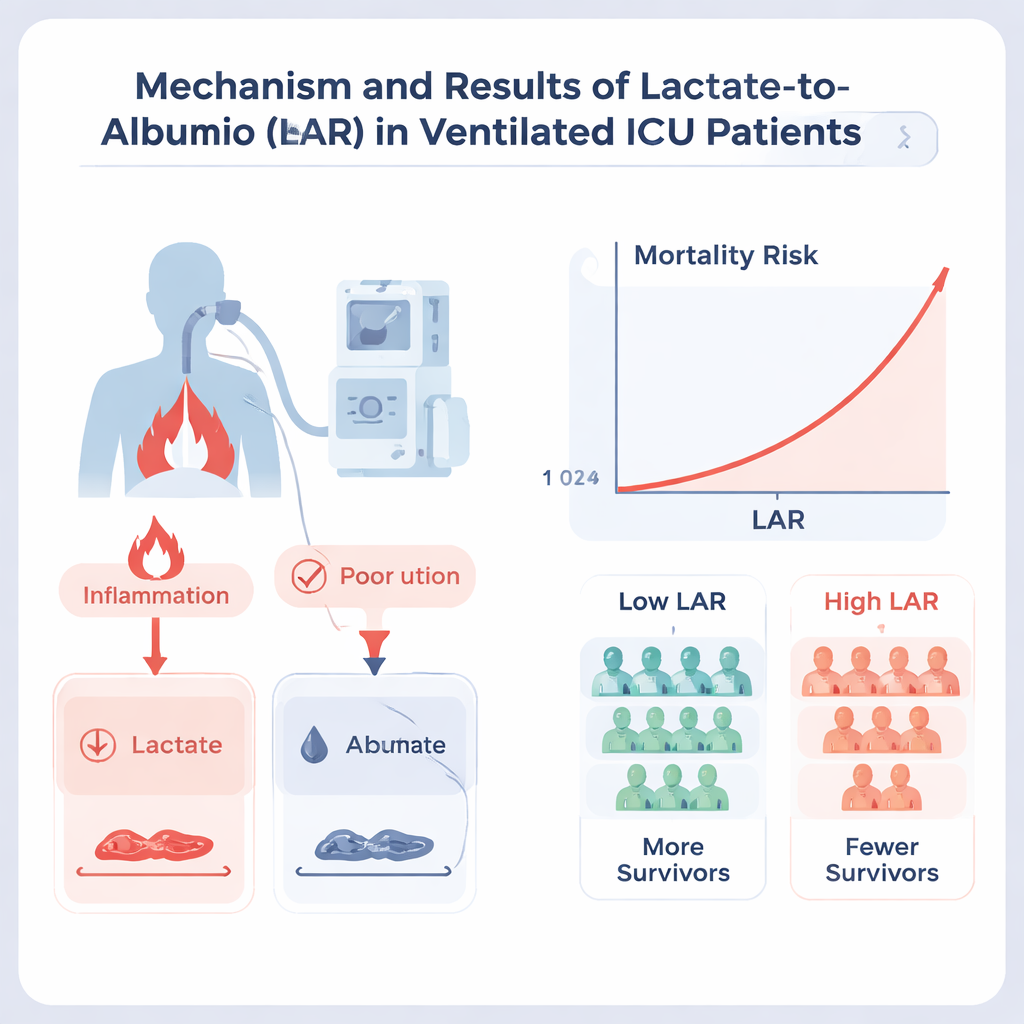
ICU teams already measure lactate and albumin for most critically ill patients. Lactate rises when tissues are starved of oxygen or under severe stress, and is often seen in shock or widespread infection. Albumin is a protein made by the liver that reflects both overall nutrition and the body’s reaction to inflammation; low levels are linked with long hospital stays and worse recovery. By dividing lactate by albumin, LAR rolls information about acute stress and long‑term health into one number. The researchers wondered if this combined measure might better capture who is most fragile among patients needing a breathing machine.
Who was studied and how
The team examined detailed electronic records from over 65,000 ICU stays at a Boston hospital, focusing on 9,195 adults who needed invasive mechanical ventilation and had lactate and albumin checked in the first 24 hours after ICU admission. They followed what happened to these patients during their ICU stay and up to one year after discharge. Patients were split into two groups using a data‑driven cut‑off LAR value of 1.48: a low‑LAR group and a high‑LAR group. The researchers then used standard statistical methods to compare death rates between these groups while accounting for age, existing illnesses, lab results, treatments received, and established ICU severity scores.
What the numbers revealed
Patients with higher LAR values were clearly sicker at the bedside: they breathed faster, had weaker blood pressures, more kidney failure, more severe infections, and worse organ‑failure scores. Their outcomes reflected this. In the high‑LAR group, nearly half died in the ICU and almost two‑thirds had died within one year, compared with about one fifth and two fifths, respectively, in the low‑LAR group. Even after adjusting for many other risk factors and scoring systems, a high LAR still meant roughly a 30% higher chance of dying both in the ICU and within a year. When LAR was treated as a sliding scale rather than a simple high‑versus‑low split, the risk of death climbed steadily as the ratio rose, with no safe “plateau” beyond which extra risk leveled off.
How this measure compares to existing tools
To see how useful LAR is next to traditional ICU scores, the authors used a machine‑learning method that ranks which variables best predict death. As expected, broad measures of chronic disease and acute illness—such as the Charlson Comorbidity Index and the Acute Physiology Score—ranked near the top. Yet LAR still emerged as an important predictor, scoring above the widely used SOFA organ‑failure score and above lactate or albumin when each was considered alone. Notably, LAR helped distinguish patients who looked similar on standard scores but went on to have very different outcomes, especially younger individuals and those without long‑standing blood or inflammatory problems.
What this means for patients and families
This study does not offer a crystal ball, and the LAR test cannot replace the careful judgment of ICU teams or comprehensive scoring systems. However, it suggests that a simple calculation based on routine blood tests can provide an extra clue about which ventilated patients are in the most danger, both immediately and over the coming year. For clinicians, it may become a quick way to spot people who need closer monitoring, earlier conversations about goals of care, or more aggressive supportive treatments. For families, understanding that such straightforward measures exist may help explain how doctors assess risk in a setting where every piece of information can matter.
Citation: Mu, Y., Lou, F., Feng, G. et al. Lactate to albumin ratio predicts one year mortality in ICU patients receiving invasive mechanical ventilation. Sci Rep 16, 5590 (2026). https://doi.org/10.1038/s41598-026-36028-w
Keywords: intensive care, mechanical ventilation, lactate albumin ratio, critical illness prognosis, ICU mortality