Clear Sky Science · en
Comparison of apparent and three-dimensional pupillary diameter measurements in cataract patients and their impact on multifocal intraocular lens selection
Why pupil size matters for cataract surgery
Cataract surgery has become one of the most common operations worldwide, and many patients now hope to come out of it with sharp distance and near vision, often without glasses. To meet these expectations, surgeons can implant advanced “multifocal” intraocular lenses that split incoming light for far and near focus. But these high-tech lenses do not work equally well for everyone. One key factor is the size of the opening in the colored part of the eye—the pupil. This study asks a deceptively simple question: are we actually measuring pupil size correctly in cataract patients, and could errors be pushing doctors toward the wrong lens choice?
Two ways to see the same pupil
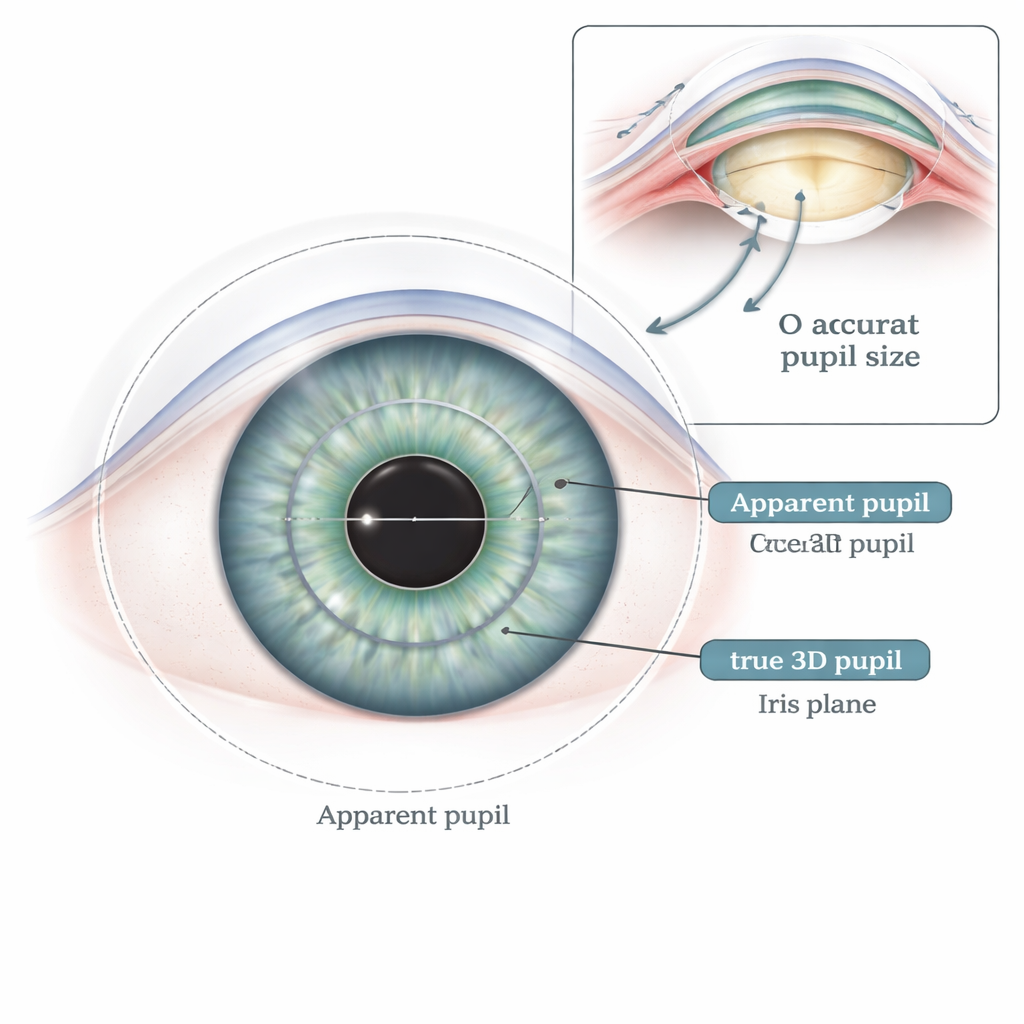
When an eye doctor looks at your pupil or measures it with common devices, they are really seeing a kind of optical illusion. Because light bends as it passes through the clear front surface of the eye (the cornea), the pupil appears slightly larger and closer to the observer than it really is. This “apparent pupil” is what most clinical tools report. In contrast, the true opening—the “real” pupil—is a three-dimensional structure sitting on the iris deeper inside the eye. The researchers used a specialized imaging system called Pentacam AXL, which can reconstruct a 3D model of the eye from many cross-sectional images. This system can measure both the usual apparent pupil and a more accurate three-dimensional pupil diameter in exactly the same sitting.
How much bigger is the apparent pupil?
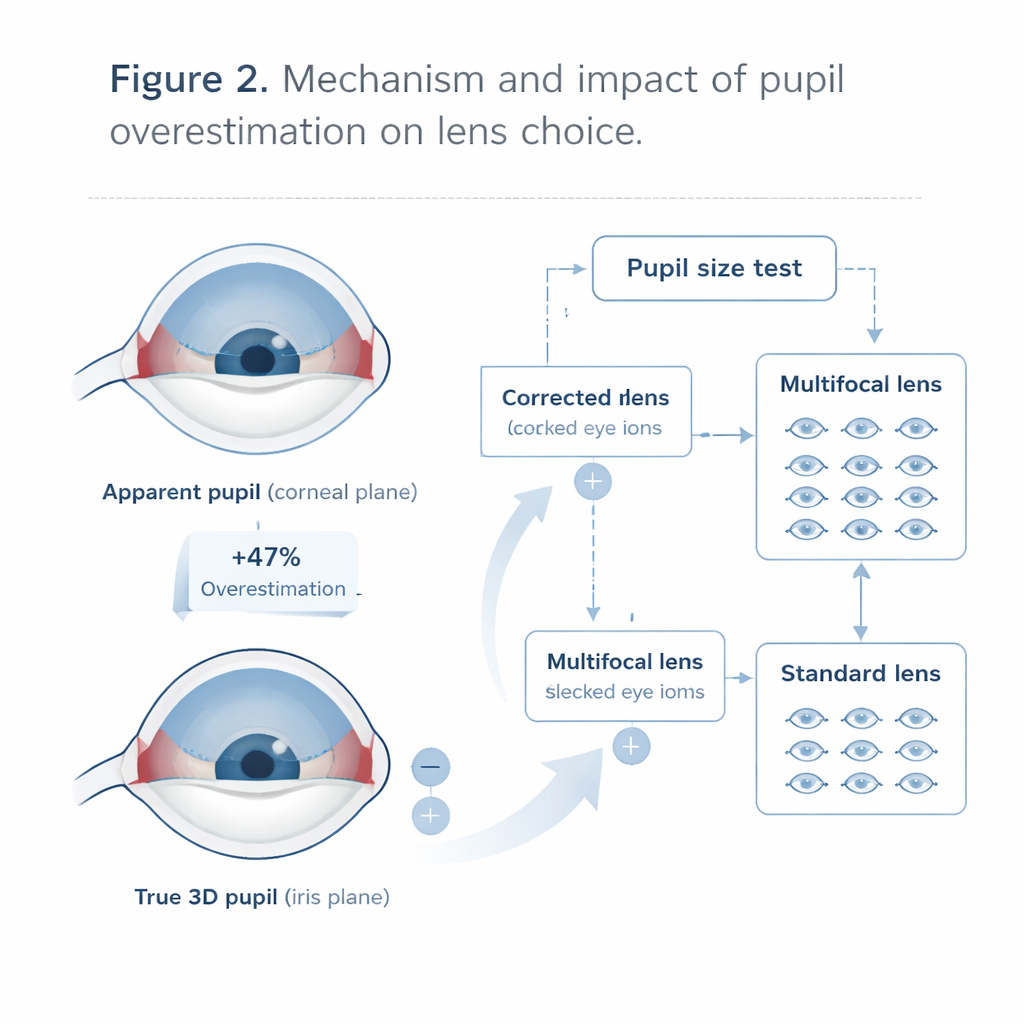
The team studied 114 eyes from 72 people with age-related cataracts, all 50 years or older. Under carefully controlled lighting, they recorded both types of pupil measurements. On average, the apparent pupil was 3.68 millimeters across, while the three-dimensional pupil measured only 2.50 millimeters. In other words, the traditional reading made the pupil look about 47 percent bigger than it really was. This magnification effect was not constant: in eyes with small pupils, the overestimate was roughly one-third, while in eyes with larger pupils it climbed to nearly two-thirds. The two measures still tracked together closely—a larger apparent pupil usually meant a larger real one—but the apparent pupil was consistently and substantially inflated.
Who is affected and what else matters?
The researchers examined whether this gap in pupil size was linked to age, sex, diabetes, or other features of the eye such as corneal thickness, length of the eye, and depth of the front chamber. They found only modest patterns. Women tended to have slightly larger apparent pupils and a greater magnification effect than men, even though their true 3D pupil size was similar. Age showed a weak tendency toward a smaller gap, likely because older eyes often have a shallower front chamber, which slightly reduces the optical magnification. Overall, however, the strongest single predictor of the three-dimensional pupil was still the apparent pupil itself, confirming that doctors can infer general trends but not exact true size from standard readings.
Consequences for choosing multifocal lenses
The most striking impact emerged when the team simulated decisions about multifocal intraocular lens (MIOL) implantation. Current expert guidelines suggest that patients should have a pupil wider than 2.8 millimeters under bright or moderate light to be good candidates for these lenses. Using the apparent pupil, 90 of the 114 eyes in the study seemed suitable. But when the same cutoff was applied to the three-dimensional pupil, only 19 eyes met the threshold. That means more than 60 percent of eyes would have been classified differently depending on which measurement was used. The study suggests that relying only on apparent pupil size may push surgeons toward multifocal lenses in many cases where the real pupil opening is smaller than believed, potentially risking reduced visual quality in dim conditions or for fine detail.
What this means for patients and surgeons
In essence, this work shows that common pupil measurements in cataract patients systematically overestimate the true opening by nearly half. For patients considering premium multifocal lenses, that distortion could matter a great deal. The authors argue that, where available, surgeons should give more weight to three-dimensional pupil measurements when judging candidacy for multifocal implants. If only traditional readings are on hand, they propose using a simple rule of thumb: divide the apparent value by about 1.47 to better approximate the true size. While further studies linking these measurements to actual post-surgery vision are needed, the message for patients is clear: not every small difference in numbers is trivial. Getting pupil size right may be a quiet but crucial step in making sure the “right” artificial lens is chosen for each individual eye.
Citation: Wang, B., Ma, H., Wang, L. et al. Comparison of apparent and three-dimensional pupillary diameter measurements in cataract patients and their impact on multifocal intraocular lens selection. Sci Rep 16, 5064 (2026). https://doi.org/10.1038/s41598-026-35975-8
Keywords: cataract surgery, pupil size, multifocal intraocular lens, eye imaging, preoperative assessment