Clear Sky Science · en
Prevalence and clinical significance of guideline-directed medical therapy in acute heart failure with reduced or mildly reduced ejection fraction
Why this matters for people with heart trouble
Heart failure is one of the leading reasons older adults end up in the hospital, and many patients are sent home on a mix of medicines meant to protect the heart. But in everyday practice, not everyone receives the full combination that guidelines recommend. This study from Japanese hospitals asked a simple but vital question: among people hospitalized for sudden worsening of heart failure, does leaving the hospital on more of these guideline-backed drugs actually translate into fewer deaths and fewer return trips to the hospital?
The people behind the numbers
The research drew on a large project called the Kyoto Congestive Heart Failure (KCHF) registry, which tracks patients admitted for acute heart failure across 19 hospitals in Japan. From more than 4,000 people, the team focused on 2,086 who had a weakened heart pump (reduced or mildly reduced ejection fraction) and survived to go home. Doctors looked at whether each patient was prescribed three major types of heart failure drugs at discharge: medicines that relax blood vessels (ACE inhibitors or ARBs), beta-blockers that slow and protect the heart, and hormone-blocking drugs called mineralocorticoid receptor antagonists. Patients were grouped by how many of these three drug types they were actually given: none, one, two, or all three.
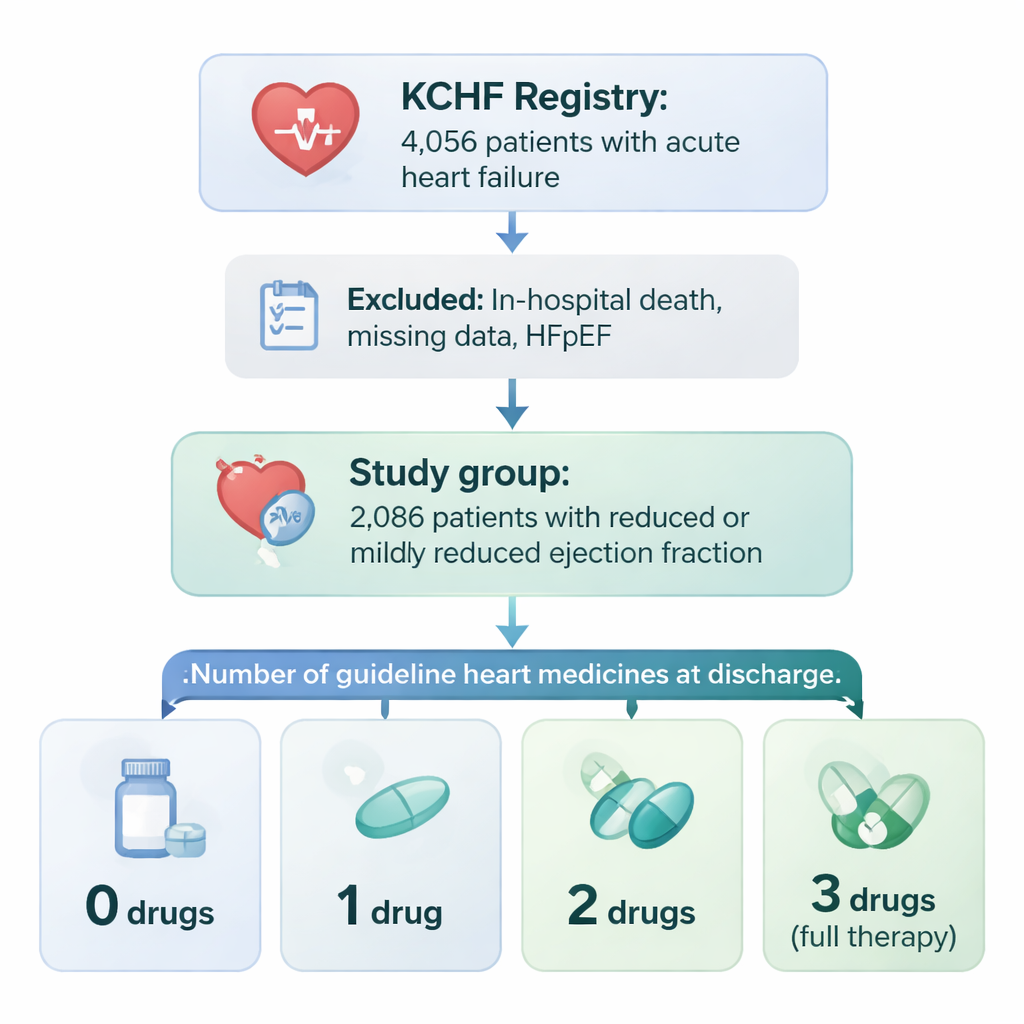
Who gets the full treatment mix
Only about three in ten patients left the hospital on all three drug classes. Those who did tended to be younger, more often male, walking independently, and with fewer serious other illnesses such as kidney failure or severe anemia. People aged 80 and older, those who came in with a heart attack, and those with badly impaired kidneys were much less likely to receive the full combination. In short, doctors were more willing or able to prescribe all three drugs to patients who looked sturdier and had fewer medical complications, and more cautious in frailer patients who might not tolerate side effects.
What happened after patients went home
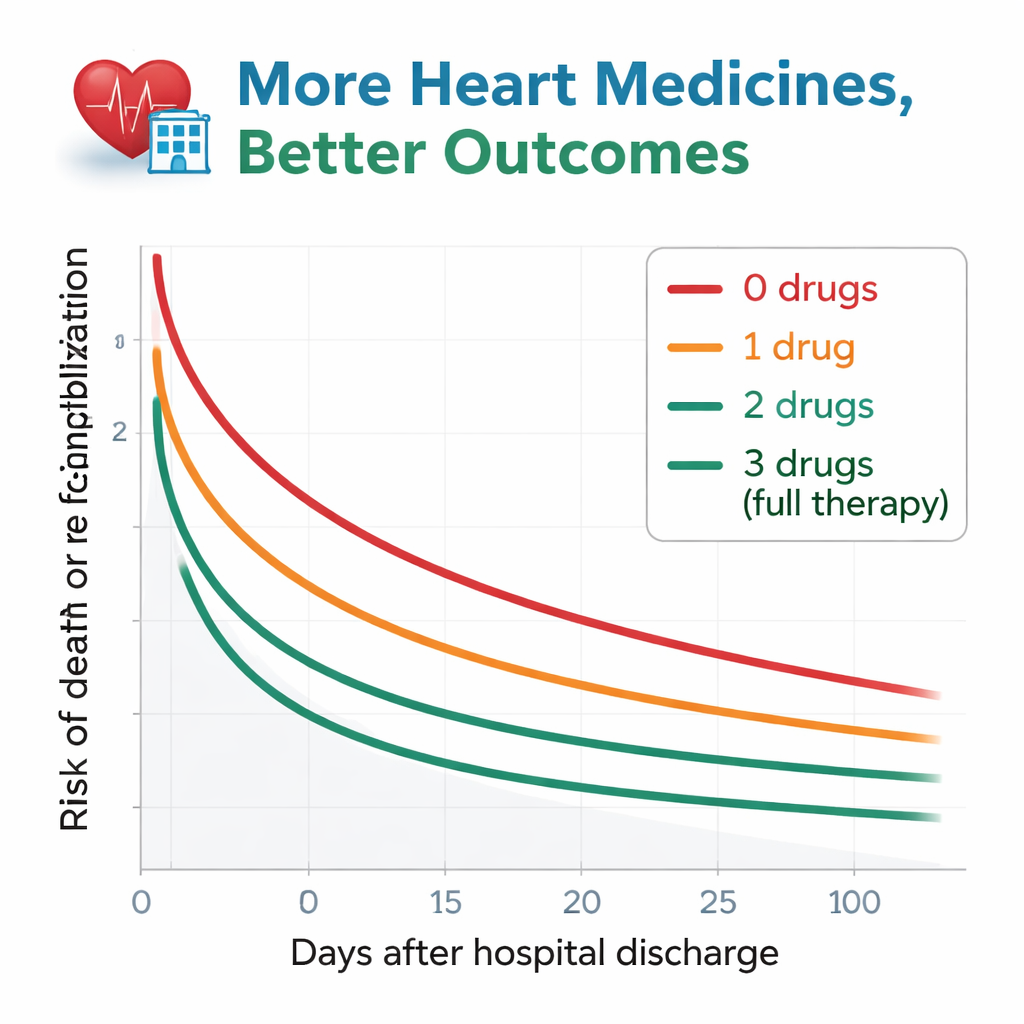
The researchers followed patients for about a year after discharge, watching for two key events: death from any cause, or being hospitalized again for worsening heart failure. The pattern was striking. Among those who received none of the guideline drugs, more than half either died or were re-admitted within a year. This risk dropped stepwise as the number of drug types increased. Patients discharged on all three had the best outcomes, with only about a quarter facing death or re-hospitalization over the same period. Even after carefully accounting for age, kidney function, anemia, and many other health factors, patients on zero or just one of the drug types still had clearly higher risk than those on all three. People on two drugs fell in between and were statistically similar to the full-treatment group.
Why some patients still miss out
The study also sheds light on why many patients do not receive the full recommended mix. Some reasons are medical: low blood pressure, kidney problems, or abnormal blood tests can make certain drugs unsafe. Older age, frailty, and difficulty taking pills regularly also play a role. Social and system issues matter too, such as how comfortable doctors are with these medicines, how closely patients can be followed after discharge, and how care varies across hospitals. The authors stress that patients who left hospital with none of the three drug types were a small but particularly vulnerable group who may have multiple barriers to treatment.
What this means for patients and families
For people living with heart failure and their caregivers, the message is straightforward: when it is safe to do so, being on more of the proven heart failure medicines seems to protect against death and repeat hospital stays. This study cannot prove cause and effect, because the sickest patients were also the least likely to receive full treatment. Still, across more than two thousand real-world cases, those discharged on all three major drug classes consistently fared better over the following year. Talking with doctors and nurses about which medicines are recommended, what side effects to watch for, and whether additional drugs can be safely added may help more patients gain the survival benefits that clinical guidelines are designed to deliver.
Citation: Miyoshi, Y., Kato, T., Morimoto, T. et al. Prevalence and clinical significance of guideline-directed medical therapy in acute heart failure with reduced or mildly reduced ejection fraction. Sci Rep 16, 5116 (2026). https://doi.org/10.1038/s41598-026-35835-5
Keywords: heart failure, guideline-directed therapy, heart medications, hospital readmission, cardiac outcomes