Clear Sky Science · en
Early prediction of pressure injury risk in hospitalized patients using supervised machine learning models based on nursing records
Why Bedsores Still Matter in Modern Hospitals
Pressure injuries—often called bedsores—may sound like an old-fashioned problem, but they remain a serious and costly complication of hospital care. They can develop quickly in people who are very ill or unable to move easily, causing pain, infection, and longer hospital stays. This study explores whether information nurses already collect in the first hours after admission can be combined with modern computer techniques to spot which patients are most likely to develop these injuries, so that staff can step in before damage occurs.
Hidden Dangers from Lying Still
A pressure injury forms when the skin and deeper tissues are squeezed between a bed or chair and the bones underneath for too long. More than one in ten hospitalized adults develop these wounds, especially those in intensive care or emergency units who cannot move freely. Beyond the pain and infection risk, these injuries carry a heavy financial burden—running into tens of billions of dollars each year in the United States alone. Traditional checklists, such as the widely used Braden Scale, help nurses estimate risk, but they can miss people whose danger is not obvious, for example those with incontinence, obesity, or complex medical problems.
Using Routine Nursing Notes as Early Warning Signals
The researchers asked whether it is possible to predict pressure injuries using only the basic information nurses routinely gather within the first eight hours of a patient’s hospital stay. At a large public hospital in Santiago, Chile, they collected data from 446 patients across many wards, from emergency and surgery to intensive care. Nurses recorded simple details such as age, height, weight, which ward the person was admitted to, how dependent they were on others for care, whether they had incontinence, and whether special mattresses, position changes, or physical restraints were being used. Any wounds already present on arrival were carefully separated from those that appeared later, so the study focused only on injuries that developed in the hospital.
Teaching Computers to Spot High-Risk Patients
From these records, the team built several “supervised” machine learning models—computer programs that learn patterns from examples. They tested five different approaches, including decision trees, logistic regression, support vector machines, extreme gradient boosting, and a popular method called Random Forest, which combines many simple decision trees into a stronger predictor. Before training the models, they cleaned and organized the raw nursing notes, filled in missing values using established statistical methods, and selected 13 of the most informative features. The data were then repeatedly split into training and testing groups to evaluate how well each model could distinguish patients who did and did not go on to develop a pressure injury.
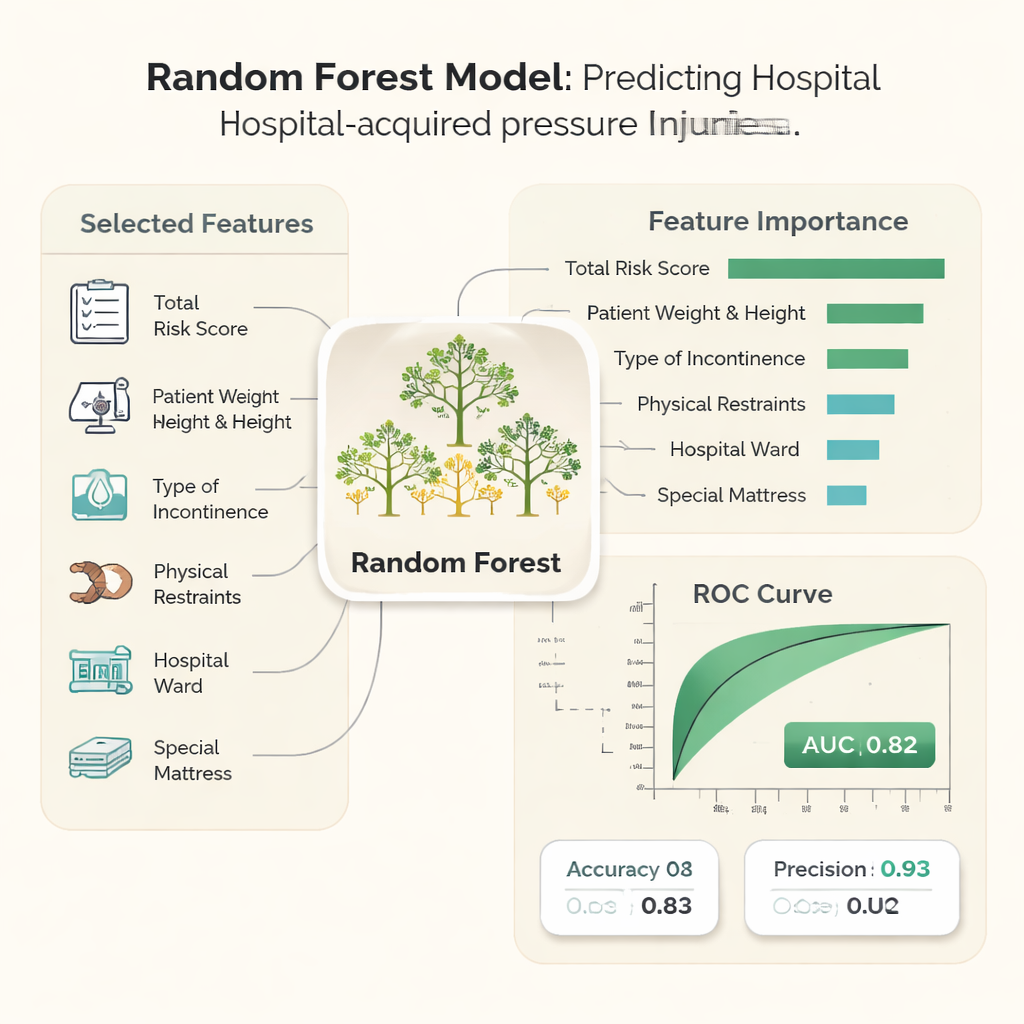
Who Is Most at Risk, According to the Data
About 19% of the patients in the study developed a hospital-acquired pressure injury. The analysis showed that some early nursing observations carried particular weight. Higher overall risk scores, greater body weight and height, high dependency on nursing care, and being admitted to certain wards, such as adult medical-surgical and intensive care units, were linked to more injuries. The presence of incontinence—especially fecal or mixed incontinence—physical restraints, and the prior use of special anti-pressure mattresses also signaled higher risk. Among the tested computer models, the Random Forest method performed best: it correctly separated high- and low-risk patients in more than four out of five cases and reached very high precision, meaning that when it flagged a patient as high risk, it was usually right.
From Computer Scores to Better Bedside Care
To make the system practical in busy wards, the researchers adjusted it to favor precision over catching every possible case. This reduces the number of false alarms, so that nurses can focus preventive resources—such as frequent repositioning, careful skin checks, and special mattresses—on those patients most likely to benefit. While this means some at-risk patients may not be flagged, the authors argue that reliable alerts are more likely to be trusted and used in day-to-day practice. They emphasize that the model is meant to support, not replace, clinical judgment.
What This Means for Patients and Hospitals
In plain terms, the study shows that hospitals could use information they already collect in the first hours after admission to power a digital “early warning system” for bedsores. With just 13 basic nursing observations and a well-trained computer model, staff can identify a small group of patients who are very likely to develop pressure injuries and intervene before serious damage occurs. Although the tool still needs to be tested in other hospitals and healthcare systems, it offers a promising way to turn routine bedside notes into smarter, more timely protection for some of the most vulnerable patients.
Citation: Barriga-Gallegos, F., Ríos-Vásquez, G., Tapia, G.M. et al. Early prediction of pressure injury risk in hospitalized patients using supervised machine learning models based on nursing records. Sci Rep 16, 6502 (2026). https://doi.org/10.1038/s41598-026-35709-w
Keywords: pressure injuries, bedsores prevention, nursing records, machine learning in hospitals, patient risk prediction