Clear Sky Science · en
The effect of preemptive use of nonsteroidal anti-inflammatory drug on inflammation, oxidative stress, and wound healing
Why timing your pain pill might matter
When we have surgery, we usually focus on how to control pain afterward. But some doctors now give pain medicine before the first cut is made, hoping to soften the body’s stress response from the start. This study asked a simple but important question: if a common painkiller is given before, after, or both before and after surgery, does it change how well bone wounds heal, or how much inflammation and “chemical stress” the body experiences?
A closer look at pain medicine and bone repair
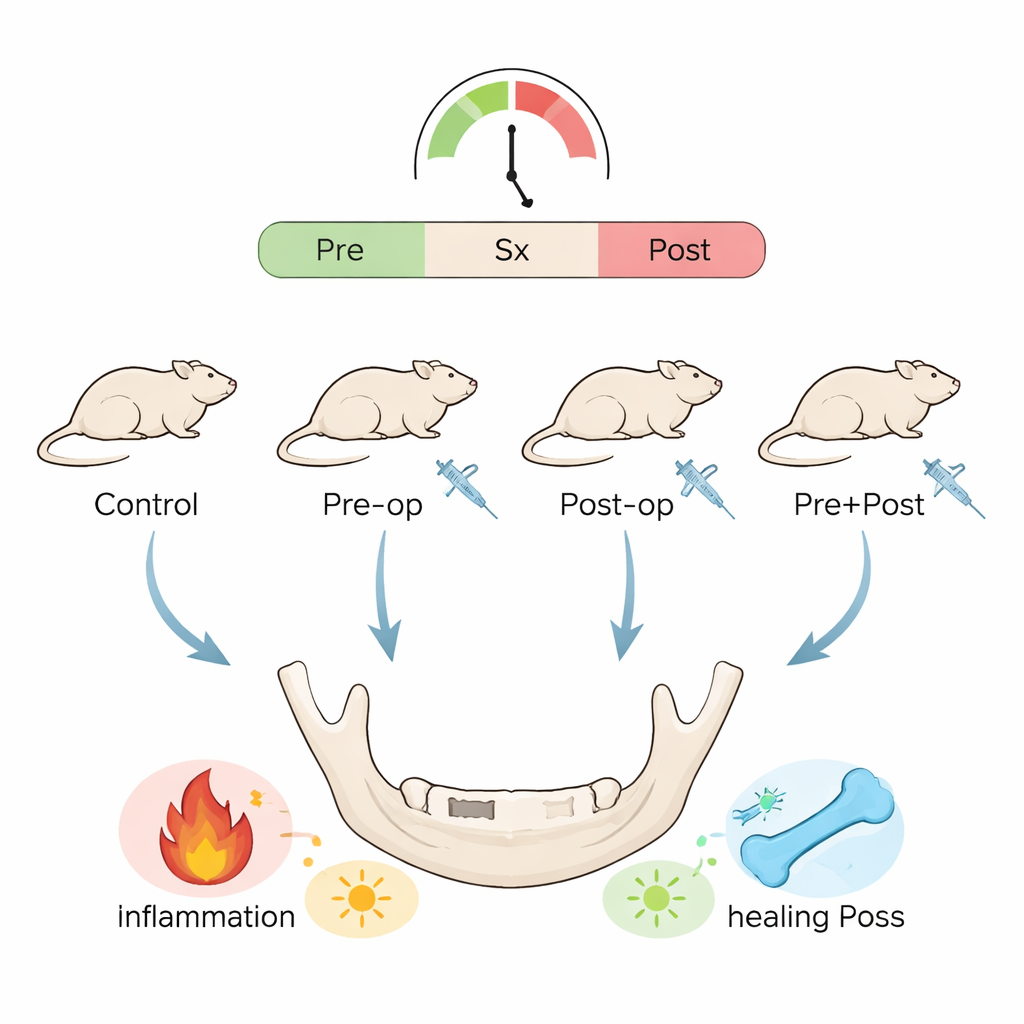
The researchers focused on a widely used painkiller called celecoxib, a type of nonsteroidal anti‑inflammatory drug (NSAID). NSAIDs are mainstays for relieving pain and swelling after dental and orthopedic procedures, but some studies suggest they might slow bone repair. To explore this, the team used 24 rats and created a small, standardized window in the lower jawbone—similar to the tiny holes surgeons make in human jawbones during plate fixation or dental implant preparation. The animals were divided into four groups: no drug, celecoxib only before surgery, celecoxib only after surgery, or celecoxib both before and after surgery.
How the experiment was set up
The drug was given by mouth for three days before surgery in the “pre‑op” groups and for three days after surgery in the “post‑op” groups. The bone defects were then allowed to heal for one, two, or four weeks. At each of these times, the scientists examined the healing bone under the microscope, counted immune cells called macrophages that help orchestrate inflammation and repair, and measured levels of signaling proteins in the blood. They also checked for markers of oxidative stress—the tug‑of‑war between damaging reactive molecules and the body’s antioxidant defenses.
What they found inside the healing bone
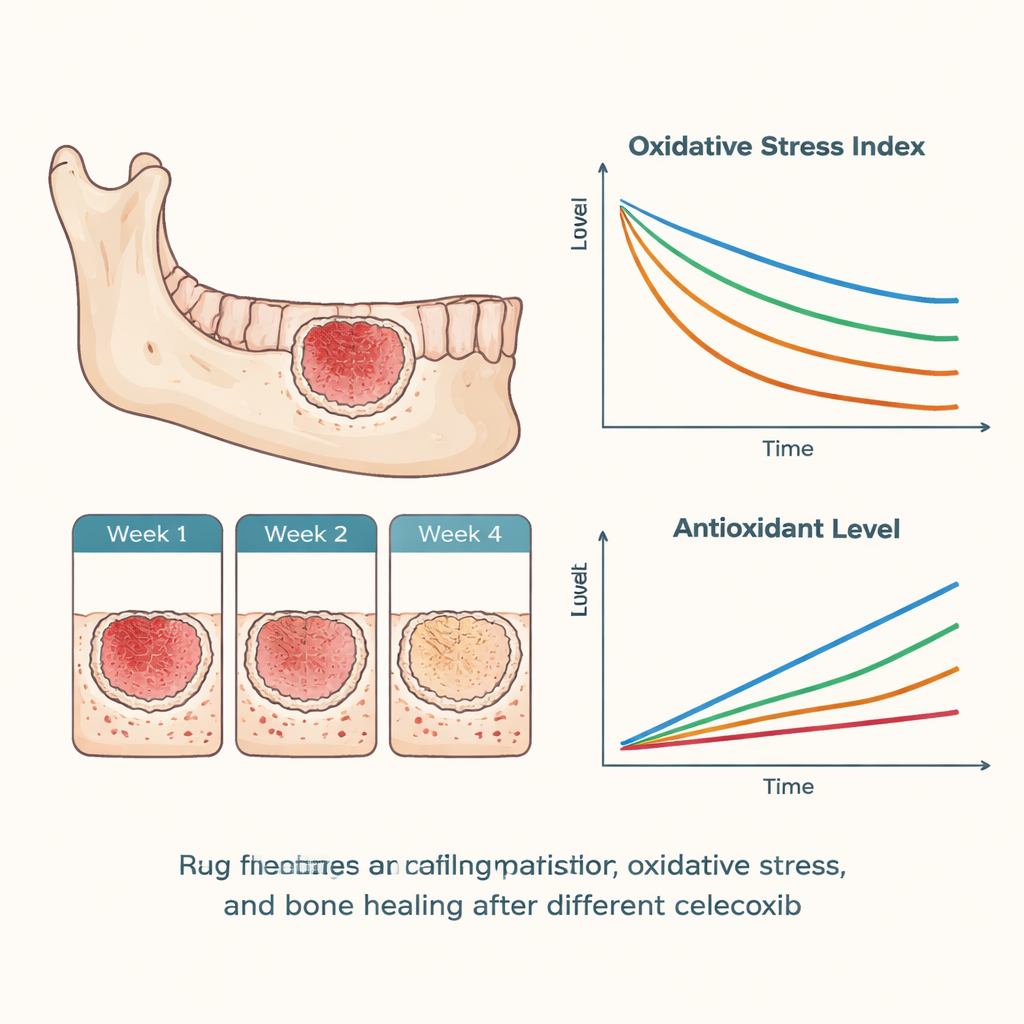
Across all groups, the jawbone defects steadily filled in with new bone over the four‑week period. Using a standard scoring system, the researchers saw minimal bone at week one, clear new bone at week two, and more advanced repair by week four. Importantly, there were no meaningful differences in these healing scores among the groups, suggesting that short‑term celecoxib—whether given before or after surgery—did not measurably harm bone regeneration in this model. Likewise, the numbers of “early‑attack” macrophages (M1 type) and “cleanup and rebuild” macrophages (M2 type) shifted over time in a broadly similar way in all groups. One subtle pattern stood out: the group that received celecoxib only after surgery showed the strongest tilt toward the pro‑inflammatory M1 type in the first week, hinting that missing pre‑surgery dosing might allow a sharper initial inflammatory surge.
Chemical signals and oxidative stress in the bloodstream
In the blood, the team tracked inflammatory messengers such as interleukins, as well as prostaglandin E₂, a key pain‑related chemical. They also measured total oxidants, total antioxidants, and an overall oxidative stress index. Statistically, most of these measures did not differ between the groups. However, one early signal was intriguing: in the first week, the pre‑surgery celecoxib group showed the highest antioxidant capacity and the lowest overall oxidative stress, while the group treated only after surgery tended toward lower antioxidant levels and higher stress. These shifts did not reach strong statistical confidence, partly because only two animals per group were examined at each time point. The authors therefore treat these findings as early hints rather than firm proof.
What this means for patients and future research
For people facing oral or facial surgery, this work offers cautious reassurance: in this rat jawbone model, short‑term celecoxib did not clearly slow bone repair. At the same time, giving the drug before surgery may gently shape the very earliest inflammatory and oxidative responses, potentially smoothing the body’s reaction to surgical injury. Because the study was intentionally small and exploratory, the authors stress that their results are not the final word. Larger, more powerful studies in animals and humans—ideally including pain scores, advanced imaging, and stronger statistics—are needed to confirm whether timing pain medicine before the first cut can both protect comfort and support healthy bone healing.
Citation: Avağ, C., Hekimoğlu, E.R., Demirci, H. et al. The effect of preemptive use of nonsteroidal anti-inflammatory drug on inflammation, oxidative stress, and wound healing. Sci Rep 16, 5152 (2026). https://doi.org/10.1038/s41598-026-35629-9
Keywords: bone healing, celecoxib, preemptive analgesia, inflammation, oxidative stress