Clear Sky Science · en
Bevacizumab enhances overall survival in newly diagnosed glioblastoma patients with high COX-2 expression
Why this brain cancer study matters
Glioblastoma is one of the deadliest brain cancers, and even with surgery, radiation, and chemotherapy, most patients live less than two years. A drug called bevacizumab can shrink tumors and ease brain swelling, but large trials suggested it does not actually help patients live longer on average. This study asks a more precise question: could a simple laboratory test on the tumor pick out a subgroup of patients who really do live longer with bevacizumab?
A closer look at a stubborn brain tumor
Glioblastoma grows quickly and is packed with abnormal blood vessels that feed the tumor. Standard treatment, often called the Stupp protocol, combines surgery to remove as much tumor as possible, followed by radiation and a chemotherapy pill named temozolomide. Bevacizumab is an antibody drug that targets a growth signal used to build new blood vessels. It is already approved in many countries for glioblastoma that has come back after treatment, and in Japan it can also be used from the start. However, because previous large trials showed that adding bevacizumab to initial treatment did not extend overall survival for the average patient, doctors have been unsure when, or even whether, to use it early.
A possible “switch” that marks more aggressive tumors
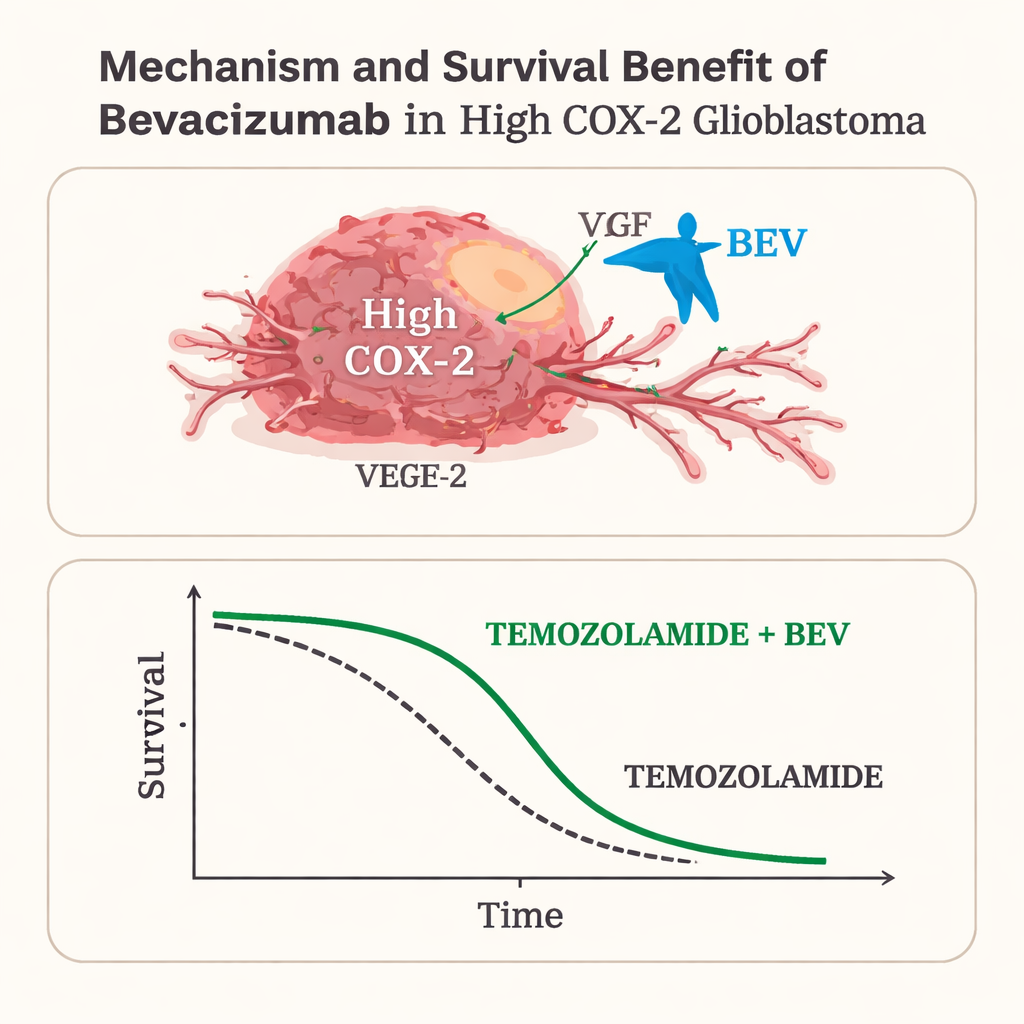
The researchers focused on a molecule called COX-2, an enzyme involved in inflammation that also helps cancers grow new blood vessels, spread, and resist drugs. High COX-2 levels in glioblastoma have long been linked to worse survival, making it a marker of particularly aggressive disease. The team wondered whether these fast-growing, highly blood‑vessel‑rich tumors might also be the ones most likely to benefit from an anti‑blood‑vessel drug like bevacizumab. To test this, they examined tumor samples from 50 adults with newly diagnosed glioblastoma treated at a single Japanese hospital between 2012 and 2023. All patients had the standard surgery, radiation, and temozolomide; some also received bevacizumab from the start.
Dividing patients by a tumor lab test
Pathologists measured COX-2 in each tumor using a staining method under the microscope, assigning an “immunoreactivity score” based on how intense the stain was and how many cells were positive. Using the median score as a cutoff, tumors were labeled either “high COX-2” or “low COX-2.” In a subset of samples, they also measured COX-2 gene activity and found that tumors with high staining generally had higher gene activity, supporting the reliability of the test. Patients were then grouped by both their COX-2 level and whether they received temozolomide alone or temozolomide plus bevacizumab, and their time to tumor regrowth and overall survival were compared.
Who really benefits from bevacizumab?
When looking at all 50 patients together, adding bevacizumab delayed tumor regrowth but did not clearly extend life, echoing earlier large trials. The picture changed sharply, however, when patients were separated by COX-2 level. Among those with high COX-2 tumors, patients who received bevacizumab lived a median of 25 months, compared with 18 months for those treated without it, and their tumors stayed under control longer as well. Statistical models that adjusted for age, functional status, and how much tumor was removed still found that bevacizumab was independently linked to better outcomes in this high COX-2 group. In contrast, among patients whose tumors had low COX-2, adding bevacizumab did not improve either the time until the cancer grew back or overall survival.
What this means for patients and health systems
For patients with high COX-2 tumors, bevacizumab appeared to erase the survival disadvantage usually associated with this aggressive biology, bringing their life expectancy close to that of patients with low COX-2 tumors. For those with low COX-2, the drug added cost and potential side effects without clear benefit. Because this was a relatively small, retrospective study from a single center, the findings need confirmation in larger, prospective trials. Still, the work suggests that a straightforward lab test on tumor tissue could help doctors target bevacizumab to the patients most likely to benefit, while sparing others an expensive and burdensome treatment that may not extend their lives.
Citation: Kesumayadi, I., Kambe, A., Kanda, H. et al. Bevacizumab enhances overall survival in newly diagnosed glioblastoma patients with high COX-2 expression. Sci Rep 16, 4974 (2026). https://doi.org/10.1038/s41598-026-35550-1
Keywords: glioblastoma, bevacizumab, COX-2, brain cancer treatment, personalized medicine