Clear Sky Science · en
Obesity as a predictor of atherogenic dyslipidemia in patients with metabolic dysfunction associated steatotic liver disease
Why belly fat and liver health matter for your heart
Many people think of fatty liver disease as a problem confined to the liver, and of obesity as mainly a weight issue. This study brings those ideas together and asks a crucial question: in people with metabolic dysfunction–associated steatotic liver disease (MASLD, formerly called non‑alcoholic fatty liver disease), does carrying extra body fat make their blood fats and blood sugar more dangerous for the heart—or are lean and obese patients equally at risk?
A common liver condition with hidden heart risks
MASLD is now one of the most widespread liver problems worldwide, affecting roughly a third of adults. Fat builds up inside liver cells and, over time, can lead to scarring and even liver cancer. But for many patients, the main threat is not liver failure; it is heart disease. Even people with MASLD who do not have diabetes or obesity show higher rates of clogged arteries and cardiovascular events. This has led researchers to ask how much of the danger comes from the liver disease itself, and how much from classic risk factors such as excess body weight. 
Taking a closer look at weight, blood fats, and sugar
To explore this, the researchers studied 452 adults aged 18 to 65 with MASLD confirmed by a noninvasive liver scan called FibroScan. All participants had at least one metabolic risk factor, such as large waist size, high blood pressure, or abnormal cholesterol. The team grouped people by body mass index (BMI) into normal weight, overweight, and obese categories. After an overnight fast, they measured blood fats, blood sugar, and insulin, and used these to calculate a set of “atherogenic indices”—combined numbers that capture how harmful a person’s cholesterol and triglyceride patterns are—and markers of how resistant the body is to insulin.
What extra weight did—and did not—change
Across the study group, only 18% of MASLD patients were lean; most were overweight or obese, and the average BMI was in the obese range. As BMI increased, insulin resistance climbed steadily and insulin sensitivity fell, showing that heavier patients’ bodies were working harder to handle sugar. Many of the combined cholesterol measures also worsened with higher BMI, meaning obese patients tended to have more “atherogenic” blood fat profiles linked to artery damage. However, when the team compared groups in detail, they found that these risky cholesterol patterns were clearly higher only in the obese patients. Overweight individuals did not differ much from normal‑weight patients on most indices. Some specific measures, such as the triglyceride–glucose index and the atherogenic index of plasma, showed only modest correlations with BMI, suggesting that weight alone cannot fully explain who has the most dangerous blood fat profile.
Fat distribution and liver disease add to the story
Body shape also mattered. BMI was strongly tied to the waist‑to‑height ratio, an indicator of belly fat that previous work has linked to heart risk in MASLD. The study’s results support the idea that central fat, insulin resistance, and fatty liver act together to drive an unhealthy mix of high triglycerides, low “good” HDL cholesterol, and small, dense LDL particles that more easily clog arteries. Yet some lean MASLD patients still showed signs of atherogenic dyslipidemia, highlighting that not all risk is visible on the scale. Other factors—such as genetics, inflammation, diet, and liver scarring—likely help determine who develops dangerous blood fat patterns. 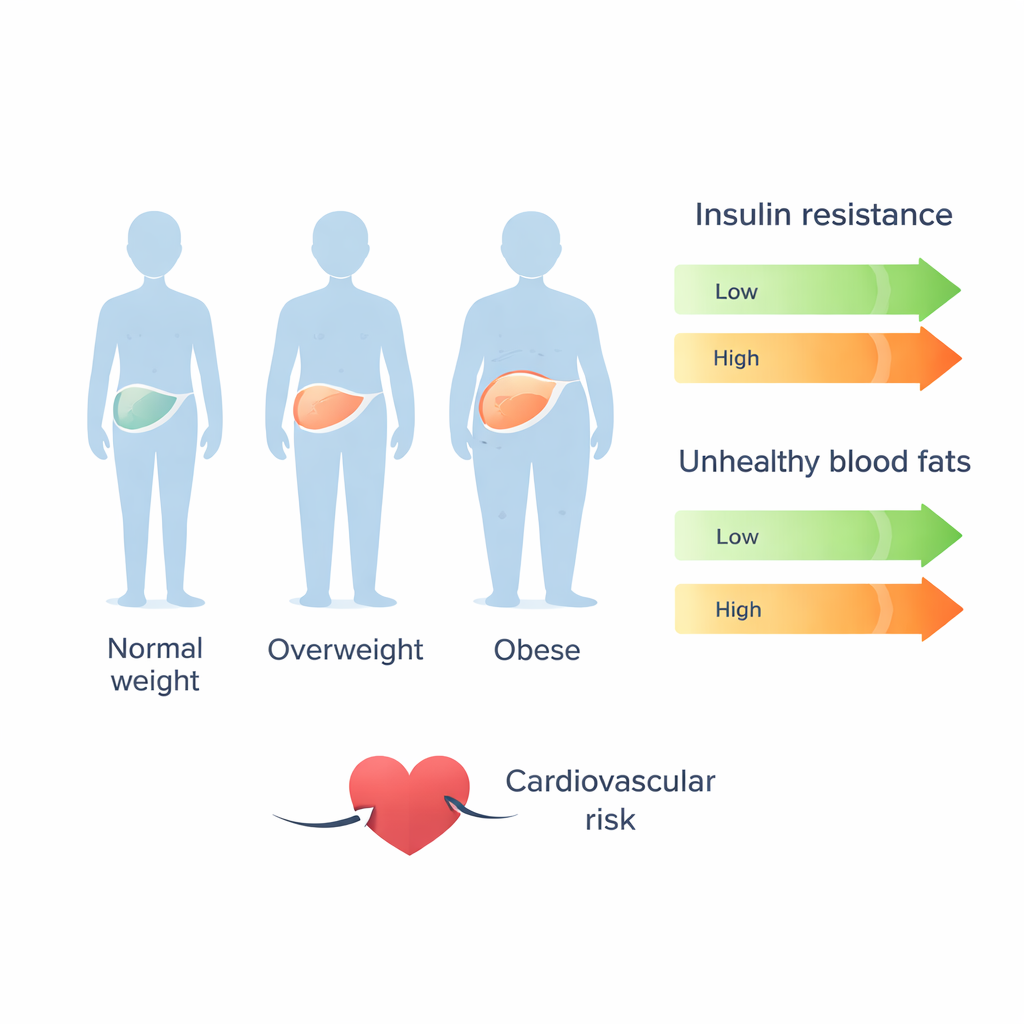
What this means for patients and care
The authors conclude that, in people with MASLD, obesity is strongly linked to worsening insulin resistance and more harmful cholesterol patterns, which together raise cardiovascular risk. Still, because some lean patients also show worrisome blood fat changes, doctors should not rely on weight alone to judge heart risk in MASLD. Instead, the study supports a more complete approach that combines careful monitoring of cholesterol and blood sugar with efforts to reduce excess weight, especially around the waist, and to improve lifestyle. For patients, the message is that managing MASLD is not just about protecting the liver: it is also a chance to lower the risk of heart attack and stroke through weight control, healthier eating, physical activity, and appropriate medical treatment.
Citation: Fotros, D., Hekmatdoost, A. & Yari, Z. Obesity as a predictor of atherogenic dyslipidemia in patients with metabolic dysfunction associated steatotic liver disease. Sci Rep 16, 6209 (2026). https://doi.org/10.1038/s41598-026-35525-2
Keywords: fatty liver disease, obesity, cholesterol, insulin resistance, heart disease