Clear Sky Science · en
Unipolar voltage map guided catheter ablation is an efficient approach to achieve pulmonary vein isolation
A Heart Rhythm Problem Many People Face
Atrial fibrillation is a common heart rhythm problem that can cause palpitations, shortness of breath and an increased risk of stroke. One major way doctors now treat it is by sealing off small blood vessels in the heart called pulmonary veins, which often trigger the abnormal rhythm. This study asks a practical question that matters to patients and doctors alike: can we make this procedure safer, quicker and just as effective by using a smarter map of the heart’s electrical signals to guide where we burn?
How Doctors Usually Tackle the Rogue Signals
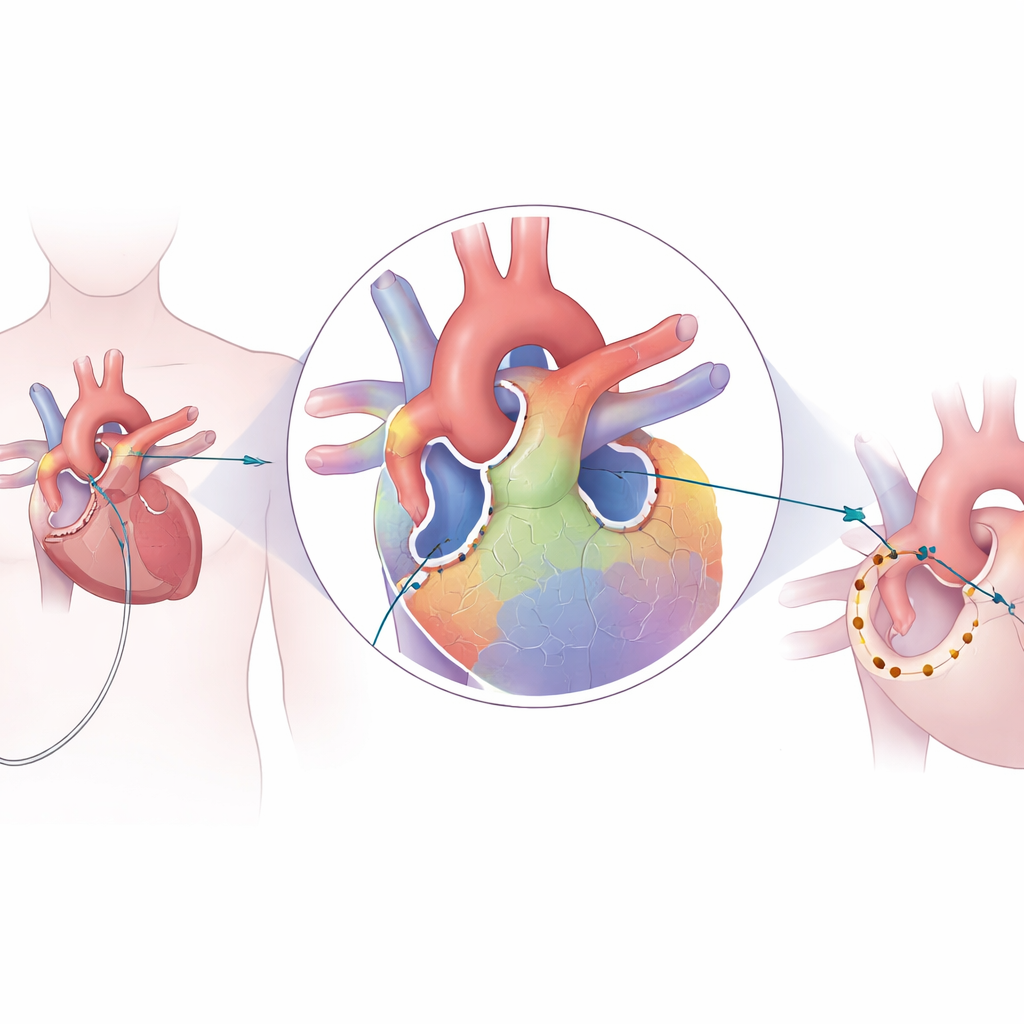
In today’s standard procedure, called pulmonary vein isolation, a thin wire is threaded through a vein in the leg up into the heart. The tip of this wire delivers heat to create tiny scars around the openings of the pulmonary veins in the left upper chamber. These scars form a continuous ring that blocks erratic electrical signals from entering the rest of the heart. Traditionally, doctors build a map of the heart’s inner surface using “bipolar” measurements, which look at the voltage between two closely spaced electrodes. They then create many closely packed burn spots around each vein until testing suggests that electrical conduction has been completely blocked.
A New Way to Read the Heart’s Electrical Landscape
The team behind this study explored whether an additional kind of map, based on “unipolar” signals, could guide a more focused treatment. Instead of comparing two neighboring points, unipolar readings reflect the voltage at a single point against a distant reference, which previous work suggests can hint at areas where the heart wall is thicker or has complex fiber layers. These thicker regions, especially around the junctions (carinas) where pulmonary veins join the atrium, are thought to be more likely to reconnect after treatment. In the new approach, the doctors first collected standard bipolar data, then adjusted the voltage scale so that these thicker areas stood out. Using this as a template, they built an unipolar voltage map that highlighted high-voltage zones presumed to be tougher tissue needing more thorough ablation.
Targeting the Tough Spots Instead of Painting the Whole Ring
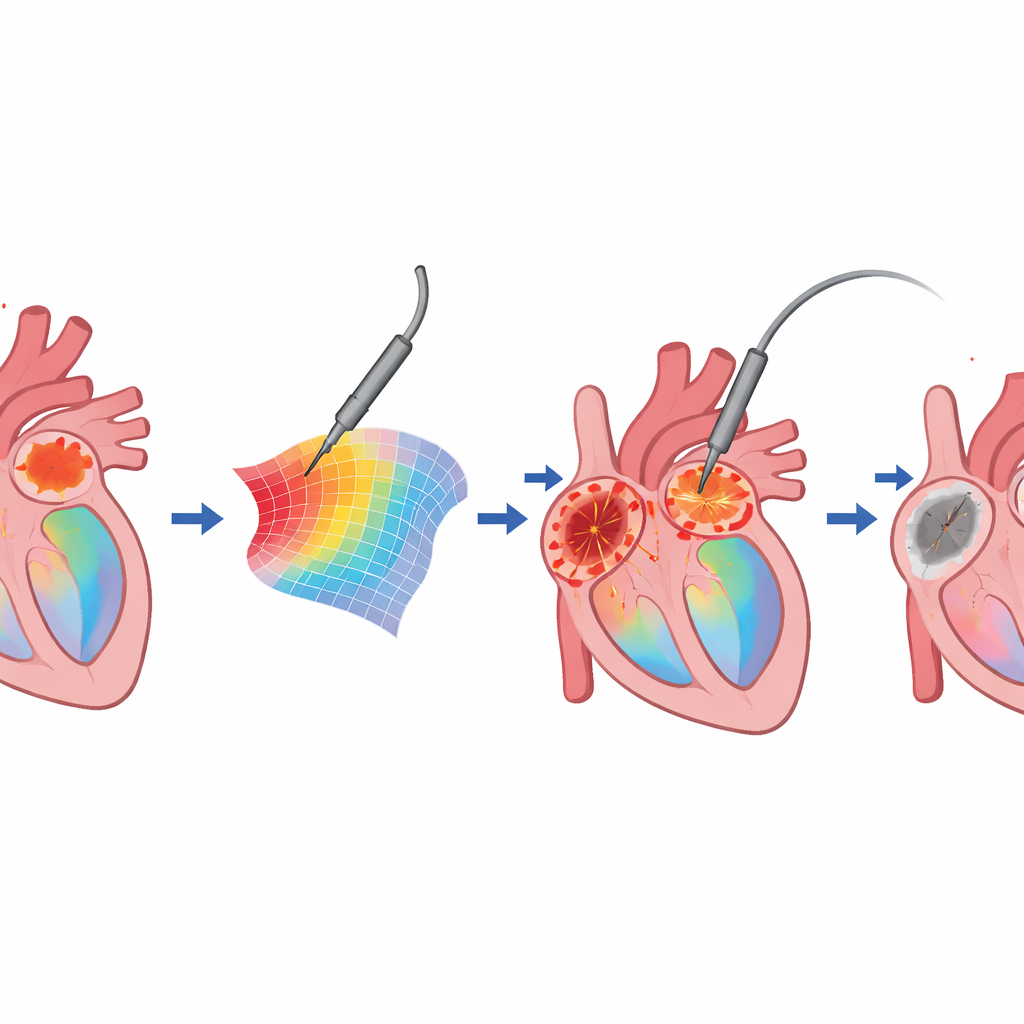
Once the unipolar map was ready, the procedure changed in a simple but important way. Rather than automatically burning all the way around each pulmonary vein in a tight circle, the doctors focused first on the zones where the voltage stayed relatively high, interpreted as thicker or more robust heart muscle. They delivered more intense applications there, while allowing greater spacing between burn spots in less demanding areas. If the pulmonary veins’ electrical signals disappeared, they stopped, even if a full visual ring of burns had not been completed. If signals persisted, they gradually adjusted the voltage range on the map to reveal any remaining high-voltage islands and treated those selectively.
What Changed in the Operating Room
The study compared 27 patients treated with the conventional method to 21 treated with the unipolar-map-guided method. Overall, both groups achieved a 100% immediate success rate in sealing off the pulmonary veins, and there were no major complications. Yet the way they got there differed. In the guided group, doctors used fewer burn points on average—about 70 instead of 97—and the total time spent delivering heat was modestly shorter. The spacing between burn spots could be larger, especially along the back wall of the atrium, even though each individual burn tended to be slightly stronger and better connected to the tissue. Importantly for patients with the intermittent (paroxysmal) form of atrial fibrillation, the proportion who remained free of documented recurrences at one year was at least as good, and possibly better, than in the conventional group, despite the reduced number of burns.
Why This Matters for Future Heart Care
Put simply, this study suggests that “smarter” targeting based on unipolar voltage maps can achieve the same goal—electrically isolating the pulmonary veins—while using fewer burn spots and concentrating energy where it is most needed. For patients, this may eventually translate into shorter procedures, fewer energy applications near sensitive structures such as the esophagus and potentially lower risk of certain complications, without sacrificing long-term rhythm control. The work is still early and comes from a single center with a modest number of patients, so larger and more balanced trials are needed. But the idea is straightforward and easy to add to existing technology, raising the possibility that future heart rhythm procedures will rely less on painting uniform rings of scar and more on tailoring treatment to the individual electrical landscape of each patient’s heart.
Citation: Matsubara, T.J., Matsumoto, S., Anai, M. et al. Unipolar voltage map guided catheter ablation is an efficient approach to achieve pulmonary vein isolation. Sci Rep 16, 8759 (2026). https://doi.org/10.1038/s41598-026-35513-6
Keywords: atrial fibrillation, pulmonary vein isolation, catheter ablation, voltage mapping, heart rhythm