Clear Sky Science · en
Superior prognostic performance of modified N staging incorporating N1c in papillary thyroid carcinoma
Why this thyroid cancer study matters
Papillary thyroid cancer is usually described as a “good” cancer because most people live a long time after diagnosis. But not everyone does equally well. This study asks a simple, important question: can we do a better job of spotting the patients whose cancer is more dangerous by looking more carefully at where it has spread to neck lymph nodes? The answer, based on data from more than 40,000 people, is yes—and the authors propose a small change to the staging system that could have big implications for treatment decisions.
Neck “zip codes” for cancer spread
When thyroid cancer spreads, it often travels first to nearby lymph nodes in the neck. Doctors divide these nodes into numbered regions, a bit like postal codes, and use them to assign an N stage, which helps guide surgery and follow-up care. The current international system groups patients into three main categories: no spread (N0), spread to central neck nodes (N1a), and spread to side-of-the-neck nodes (N1b). However, earlier research hinted that not all involved regions carry the same risk, even when they are placed in the same group. In particular, spread to three distant areas—under the jaw (level I), low in the back of the neck (level Vb), and just below the neck in the upper chest (level VII)—may signal a more aggressive cancer than spread to other neck nodes.
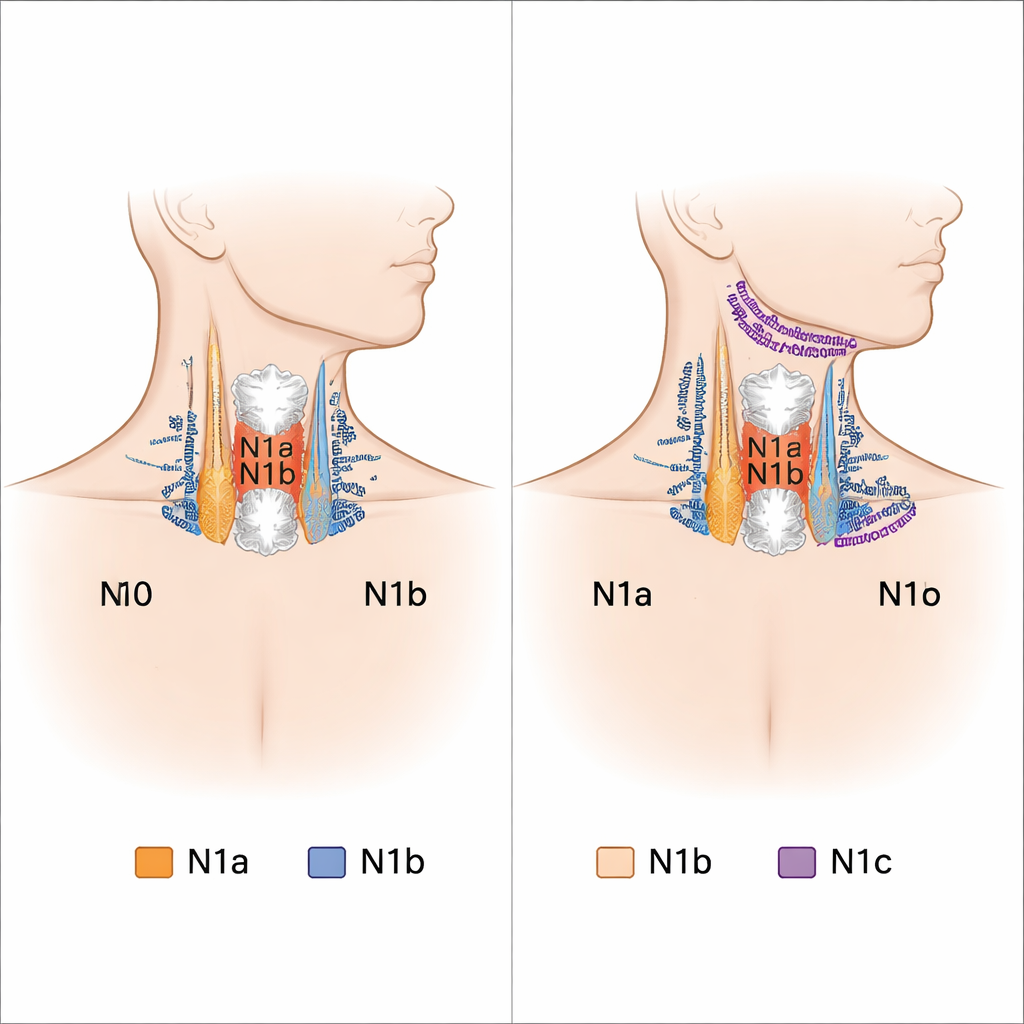
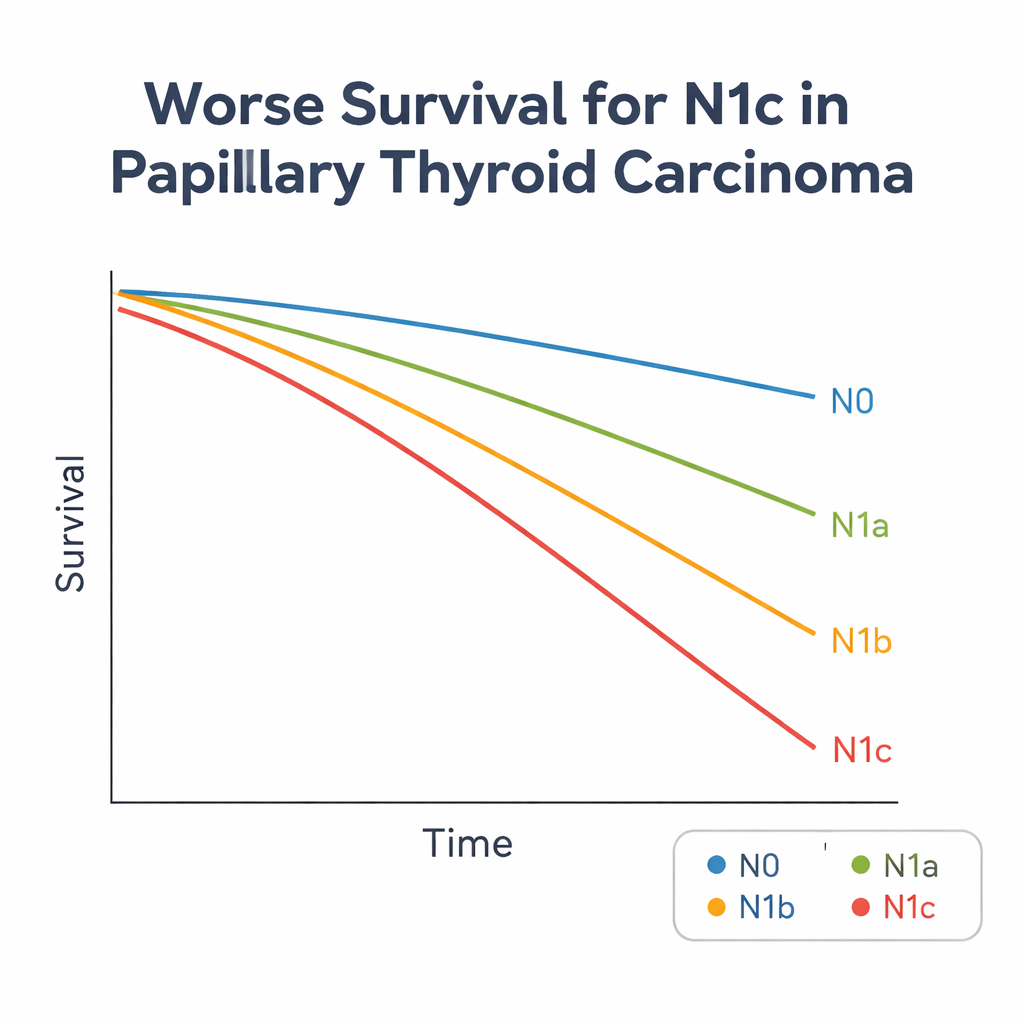
A new high‑risk group called N1c
To test this idea, the researchers used the U.S. SEER cancer registry to analyze 40,371 people with papillary thyroid cancer diagnosed between 2004 and 2015. They compared cancer-specific survival—that is, the chance of dying from thyroid cancer rather than other causes—for patients with lymph node spread in different neck regions. Even after adjusting for age, sex, tumor size, and other factors, patients with cancer in levels I, Vb, or VII had very similar and clearly worse survival than those with spread to more typical neck regions. The authors grouped these three areas into a new category they call N1c and compared it with N0, N1a, and the remaining N1b patients. Patients in this N1c group had the poorest outcomes, with more than five times the risk of dying from thyroid cancer compared with those who had no involved nodes.
What makes N1c patients different
The study also looked at what set N1c patients apart clinically. Compared with others, they tended to be younger and more often male, had larger tumors, more frequent growth of the cancer outside the thyroid, and cancer present in multiple spots within the gland. They also had more positive lymph nodes, more distant spread outside the neck, and more advanced overall stage. Using statistical models, the authors found that being male, having a larger tumor, growth beyond the thyroid, and multiple tumor foci all independently raised the odds of having N1c-type spread. In other words, the new group captures a cluster of unfavorable features that together point to a more advanced disease process.
Better prediction with a simple tweak
To see whether their proposal truly improves risk prediction, the researchers compared the modified four-level system (N0, N1a, N1b, N1c) with several established ways of staging lymph node disease, including the current American Joint Committee on Cancer N system and more complex methods based on the number or proportion of positive nodes. Using standard measures of predictive accuracy, the new scheme performed best at forecasting thyroid cancer deaths. Importantly, it does this using information that surgeons and pathologists already collect: which neck levels are involved. The authors also link their findings to day-to-day surgical dilemmas, such as how far up or down the neck and chest surgeons should go when removing lymph nodes, arguing for a targeted rather than routine removal of these high‑risk regions while paying close attention to patients with N1c risk factors.
What this means for patients and doctors
For people with papillary thyroid cancer, the study does not change the basic fact that most will live long, healthy lives. But it suggests that a relatively small group—about 3% of patients, but more than a quarter of those with side-of-the-neck spread—face a higher risk than their current stage might suggest. By carving out this N1c group, doctors could more accurately identify who might benefit from more extensive lymph node surgery, closer imaging follow-up, or additional treatments such as radioactive iodine, while sparing lower-risk patients from unnecessary procedures. In short, a modest refinement of the lymph node staging map may offer a clearer forecast of the road ahead for people living with papillary thyroid cancer.
Citation: Ouyang, H., Li, X., Dou, X. et al. Superior prognostic performance of modified N staging incorporating N1c in papillary thyroid carcinoma. Sci Rep 16, 4998 (2026). https://doi.org/10.1038/s41598-026-35461-1
Keywords: papillary thyroid cancer, lymph node staging, neck metastasis, cancer prognosis, thyroid surgery