Clear Sky Science · en
A system for invitro inhaled/exhaled aerosol testing of personal protective equipment
Why this study matters for everyday life
During the COVID-19 pandemic, people were told to wear masks, keep their distance, and sometimes use face shields, yet it has remained surprisingly hard to compare how well these options actually block tiny airborne particles. This study describes a laboratory test system that mimics one person exhaling virus‑like aerosols and another person breathing them in, and then measures how different masks, shields, and distances change the amount of material that reaches the “receiver.” The work does not rank brands or give medical advice, but it helps clarify broad questions many people have: Do shields work as well as masks? Does distance really matter? And what happens when both people mask up?
Building a safe way to test risky air
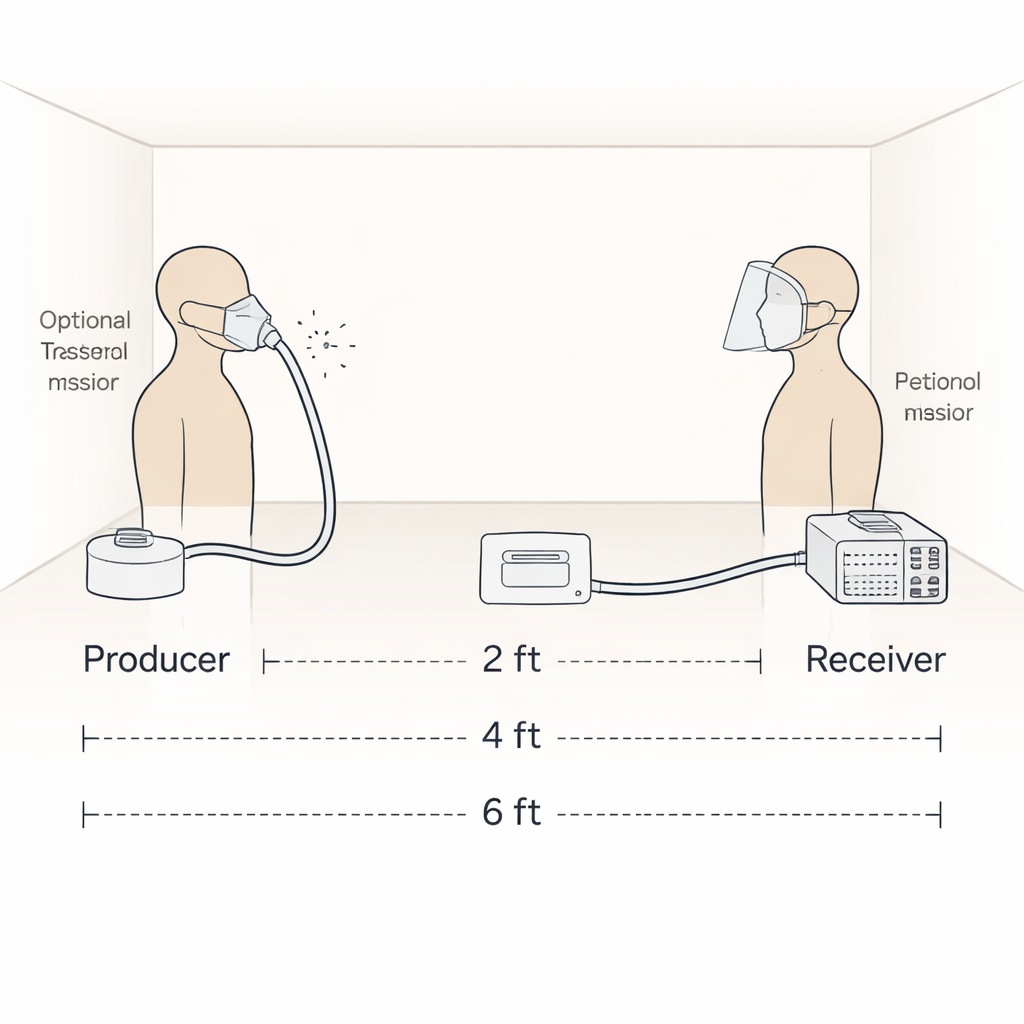
To explore these questions without putting anyone at risk, the researchers built an in‑vitro system using two life‑sized manikin heads in a small, low‑ventilation room. One manikin acted as the aerosol producer. Medical air was pumped through a nebulizer containing salty water, generating a mist of tiny droplets similar in size to those we release when breathing, speaking, coughing, or sneezing. This mist was routed into the manikin’s airway so that visible “exhaled” aerosols emerged from its nose and mouth. The other manikin, the receiver, was fitted with a sensitive optical particle counter positioned at the mouth and connected to a simple mechanical ventilator that imitated human breathing. In this way, the team could track, second by second, how much particulate matter smaller than 5 micrometers reached the receiver under tightly controlled conditions.
Trying out common masks and shields
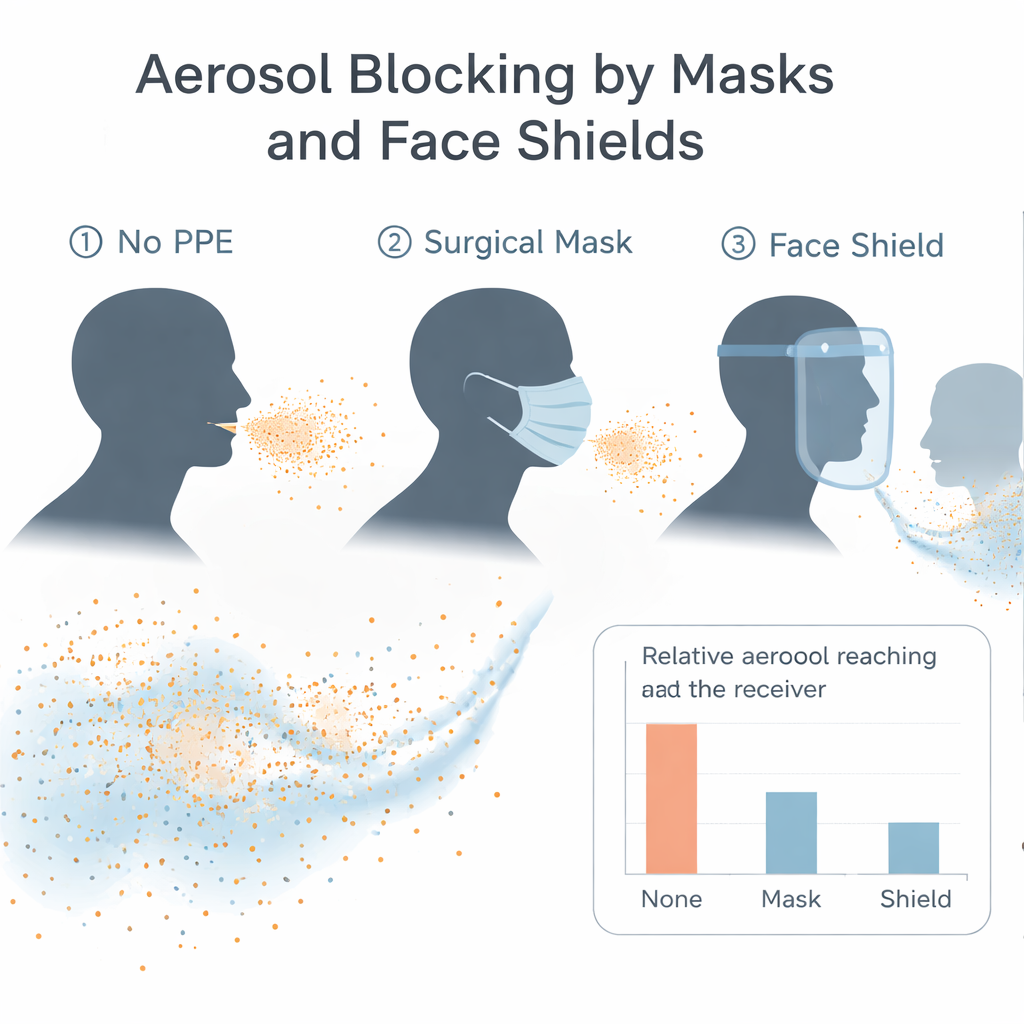
The team examined nine kinds of personal protective equipment (PPE): several types of masks, including surgical masks, N95 and KN95 respirators, a washable cloth mask, and a mask with an attached shield, plus three stand‑alone face shields of different designs. They ran three main sets of experiments. First, they placed PPE on the aerosol‑producing manikin and left the receiver unprotected. Second, they reversed this, masking or shielding only the receiver. Third, they put a disposable medical mask on both manikins. For each setup, the manikins were placed 2, 4, or 6 feet apart, and the producer could face the receiver directly or at 45‑ or 90‑degree angles. Each test lasted five minutes and was repeated three times to check consistency.
What the particles revealed
Ultraviolet photos using a fluorescent solution showed where larger droplets escaped from the different devices, but the key findings came from the particle measurements. In general, masks on the aerosol producer reduced the amount of fine particles that reached the receiver, especially at 6 feet, where most PPE kept levels close to the background in the room. However, performance varied: a standard disposable medical mask tended to block more aerosols than shields or some cloth designs. Surprisingly, at the closest distance of 2 feet, several configurations, such as using a KN95 or a washable cloth mask on the producer with no barrier on the receiver, sometimes resulted in higher detected levels than using no PPE at all. The authors suggest that in a small, poorly ventilated room, deflected plumes and recirculation can concentrate aerosols in unexpected spots rather than indicating true failure of the devices themselves. Changing the angle between the manikins also altered exposures for some PPE, because leaks around the nose, cheeks, and under shields can redirect plumes sideways or downward.
Masks versus shields and the power of double masking
When PPE was placed on the receiving manikin instead, masks again performed better overall than the shields tested. In this configuration, some shields actually appeared to “collect” and funnel aerosols toward the receiver, producing particle levels that exceeded those measured with no protection at all at certain distances. The standout scenario was the simplest: when both manikins wore disposable medical masks and faced each other at 2, 4, or 6 feet, the aerosols detected at the receiver dropped to near background levels, showing a strong combined effect of source control plus wearer protection. Across conditions, increasing the distance between producer and receiver consistently reduced exposure, reinforcing the value of physical spacing alongside masking.
What this means for real‑world protection
This test system has limitations: it uses nebulized saline rather than true respiratory fluid, relies on manikins that cannot perfectly match human faces or mask fit, and was run in a single small room. The authors emphasize that their results should be viewed as relative patterns, not exact predictions for every real‑world setting or product. Still, the message for non‑specialists is clear. In this controlled model, ordinary medical masks did a better job than the sampled shields at limiting tiny airborne particles, and having both people wear masks, especially with some distance between them, pushed exposures down close to the room’s natural background. The study offers a practical framework for designing more advanced tests in the future and supports everyday advice many people now follow instinctively: keep your distance when you can, and when sharing air indoors, simple well‑fitted masks on everyone go a long way toward reducing what you breathe in.
Citation: Baldelli, A., Poznikoff, A. & Purdy, R. A system for invitro inhaled/exhaled aerosol testing of personal protective equipment. Sci Rep 16, 5535 (2026). https://doi.org/10.1038/s41598-026-35248-4
Keywords: face masks, face shields, aerosol transmission, social distancing, COVID-19